Mis à jour le Mercredi, 14 Avril 2021

Source: An Introduction to Developmental Psychology by Slater & Bremner (Blackwell:Oxford, 2nd Edn, 2011)
It is fundamental to undertstand that as human beings, whatever stage of our lives we are, in order to be able to function fully in our daily lives and in any other activity we first of all need to have a strong foundation. That foundation is our brain, and hence, if our brain [i.e. the hardware] is not physiologically within the limits of what is deemed fit and healthy, every aspect of our mind will be affected and also of our lives. There is no psyche [mind] without a brain, because this biological hardware given to us by nature throughout the course of the shared evolutionary history of primates on planet Earth, allows us to experience every aspect of our lives, both physical and psychical [i.e. mental].
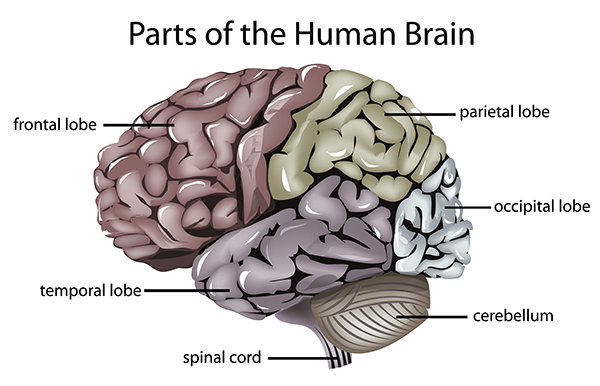
So, before diving deeper into the depth of children’s development, we are going to explore this link between brain and behaviour in order to get a foundation of the importance or a healthy brain, for a healthy development and a healthy and fulfulling life, by starting with how brain damage can affect our personalities and mental abilities; we are going to look at the Frontal lobe, which is the part of the brain behind our forehead responsible for problem solving, strategic planning, use of environmental instructions to shift procedures, and the inhibition of impulsivity.

(Photo: Jez C Self / Frontal Lobe Gone)
Frontal Lobes (& Frontal Lobe Damage)
The Wisconsin Card Sorting Test (WCST; Grant & Berg, 1948; Heaton, Chelune,Talley, & Curtis, 1993) has long been used in Neuropsychology and is among the most frequently administered neuropsychological instruments (Butler, Retzlaff, & Vanderploeg, 1991).
The test was specifically devised to assess executive functions mediated by the frontal lobes such as problem solving, strategic planning, use of environmental instructions to shift procedures, and the inhibition of impulsivity. Some neuropsychologists however, have questioned whether the test can measure complex cognitive processes believed to be mediated by the Frontal lobes (Bigler, 1988; Costa, 1988).
The WCST test, until this day remains widely used in clinical settings as frontal lobe injuries are common worldwide. Performance on the WCST test is believed to be particular sensitive in reflecting the possibilities of patients having frontal lobe damage (Eling, Derckx, & Maes, 2008). On each Wisconsin card, patterns composed of either one, two, three or four identical symbols are printed. Symbols are either stars, triangle, crosses or circles; and are either red, blue, yellow or green.
At the start of the test, the patient has to deal with four stimulus cards that are different from one another in the colour, form and number of symbols they display. The aim of the participant would be to correctly sort cards from a deck into piles in front of the stimulus cards. However, the participant is not aware whether to sort by form, colour or by number. The participant generally starts guessing and is told after each card has been sorted whether it was correct or incorrect.
Firstly they are generally instructed to sort by colour; however as soon as several correct responses are registered, the sorting rule is changed to either shape or number without any notice, besides the fact that responses based on colour suddenly become incorrect. As the process continues, the sorting principle is changed as the participant learns a new sorting principle.
 It has been noted that those with frontal lobe area damage often continue to sort according to only one particular sorting principle for 100 or more trials even after the principle has been deemed as incorrect (Demakis, 2003). The ability to correctly remember new instructions with for effective behaviour is near impossible for those with brain damage: a problem known as ‘perseveration’.
It has been noted that those with frontal lobe area damage often continue to sort according to only one particular sorting principle for 100 or more trials even after the principle has been deemed as incorrect (Demakis, 2003). The ability to correctly remember new instructions with for effective behaviour is near impossible for those with brain damage: a problem known as ‘perseveration’.
Another widely used test is the ‘Stroop Task’ which sets out to test a patient’s ability to respond to colours of the ink of words displayed with alternating instructions. Frontal patients are known for badly performing to new instructions. As the central executive is part of the frontal lobe, other problems such as catatonia – a condition where patients remain motionless and speechless for hours while unable to initiate – can arise. Distractibility has also been observed, where sufferers are easily distracted by external or internal stimuli. Lhermite (1983) also observed the ‘Utilisation Syndrome’ in some patients with Dysexecutive Syndrome (Normal & Shallice, 1986), who would grab and use random objects available to them pathologically.
Incomplete Frontal Lobe Development & Impulsiveness in Children

Image: PsyBlog
The Frontal lobe, responsible for most executive functions and attention, has shown to take years [at least 20] to fully develop. The Frontal lobe [located behind the forehead] is responsible for all thoughts and voluntary behaviour such as motor skills, emotions, problem-solving and speech.
In childhood, as the frontal lobe develops, new functions are constantly added; the brain’s activity in childhood is so intense that it uses nearly half of the calories consumed by the child in its development.
As the Pre-Frontal Lobe/Cortex is believed to take a considerable amount of at least 20 years to reach maturity (Diamond, 2002), children’s impulsiveness seem to be linked to neurological factors with the Pre-Frontal Lobe/Cortex; particularly, their [sometimes] inability to inhibit response(s).
The idea was supported by developmental psychologist and philosopher Jean Piaget‘s Theory of Cognitive Development of Children [known for his epistemological studies] where he showed the A-not-B error [also known as the “stage 4 error” or “perseverative error”] is mostly made by infants during the substage 4 of their sensorimotor stage.
Researchers used 2 boxes, marked A and B, where the experimenter had repeatedly hid a visually attractive toy under the Box A within the infant’s reach [for the latter to find]. After the infant had been conditioned to look under Box A, the critical trial had the experimenter move the toy under Box B.
Children of 10 months or younger make the “perseveration error” [looked under Box A although fully seeing experimenter move the toy under Box B]; demonstrating a lack of schema of object permanence [unlike adults with fully developed Frontal lobes].

Frontal lobe development in adults was compared with that in adolescents, e.g. Sowell et al (1999); Giedd et all (1999); who noted differences in Grey matter volume; and differences in White matter connections. Adolescents are likely to have their response inhibition and executive attention performing less intensely than adults’. There has also been a growing & ongoing interest in researching the adolescent brain; where great differences in some areas are being discovered.
The Pre-Frontal Lobe/Cortex [located behind the forehead] is essential for ‘mentalising’ complex social and cognitive tasks. Wang et al (2006) and Blakemore et al (2007) provided more evidence between the difference in Pre-Frontal Lobe activity when ‘mentalising’ between adolescents and adults. Anderson, Damasio et al (1999) also noted that patients with very early damage to their frontal lobes suffered throughout their adult lives.

2 subjects with Frontal Lobe damage were studied:
1) Subject A: Female patient of 20 years old who suffered damages to her Frontal lobe at 15 months old was observed as being disruptive through adult life; also lied, stole, was verbally and physically abusive to others; had no career plans and was unable to remain in employment.
2) Subject B was a male of 23 years of age who had sustained damages to his Frontal lobe at 3 months of age; he turned out to be unmotivated, flat with bursts of anger, slacked in front of the television while comfort eating, and ended up obese in poor hygiene and could not maintain employment. [However…]
Reflections
While research and tests have proven the link between personality traits & mental abilities and frontal brain damage, the physiological defects of the frontal lobe would likely be linked to certain traits deemed negative by a subject willing to be a functional member of society [generally Western societies].
However, personality traits similar to the above Subjects [A & B] may in fact not always be linked to deficiency and/or damage to the frontal lobes; as many other factors are to be considered when assessing the behaviour & personality traits of subjects; where [for example] violence and short temper may [at times] be linked to a range of factors and environmental events during development, or other mental strains such as sustained stress, emotional deficiencies due to abnormal brain neurochemistry, genetics, or other factors that may lead to intense emotional reactivity [such as provocation or certain themes/topics that have high emotional salience to particular subjects, ‘passion‘]
THE 3 MAJOR THEORIES OF DEVELOPMENT
In 1984, Nicholas Humphrey described us as “nature’s psychologists’” or homo psychologicus. What he meant was that as intelligent social beings, we tend to use our knowledge of our own thoughts and feelings – “introspection” – as a guide for understanding how others are likely to think, feel and hence, behave. He also argued that we are conscious [i.e. we have self-awareness] precisely because such an attribute is useful in the process of understanding others and having a successful social existence – consciousness is a biological adaptation that enables us to perform introspective psychology. Today, we are confident in the knowledge that the process of understanding others’ thoughts, feelings and behaviour is an ability that develops through childhood and most likely throughout our lives; and according to the greatest child psychologist of all time, Jean Piaget, a crucial phase of this process occurs in middle childhood.
Developmental psychology can be characterised as the field that attempts to understand and explain the changes that happen over time in the thought, behaviour, reasoning and functioning of a person due to biological, individual and environmental influences. Developmental psychologists study children’s development, and the development of human behaviour across the organism’s lifetime from a variety of different perspectives. Hence, if we are studying different areas of development, different theoretical perspectives will be fundamental and may influence the ways psychologists and scholars think about and study development.
Through the systematic collection of knowledge and experiments, we can develop a greater understanding and awareness of ourselves than would otherwise be possible.
Focussing on changes with time
The new born infant is a helpless creature, with communications skills that are limited along with few abilities. By 18 – 24 months, the end of the period of infancy – this scenario changes. The child has now formed relationships with others, has gained knowledge about the aspects of the physical world, and is about to undergo a vocabulary explosion as language development leaps ahead. At the time of adolescence, the child has turned into a mature, thinking individual actively striving to come to terms with a fast changing and complex society.
The important contribution to development, is maturation and the changes resulting from experience that intervene between the different ages and stages of childhood: the term maturation refers to those aspects of development that are primarily under genetic control, and which are relatively uninfluenced by the environment. An example would be puberty, and although its onset can be affected by environmental factors such as diet, the changes that occur are genetically determined.
Development Observed
The biologist, Charles Darwin, notable for his theory of evolution, made one of the earliest contributions to our understanding of child psychology in his article “A biographical sketch of an infant” (1877), which was based on observations of his own son’s development. By the early 20th century, most of our understanding of psychological development was not based on scientific methodology as much was still based on anecdotes and opinions of qualitative analysis, a method that strict empiricists have never managed to grasp or like. Nevertheless, knowledge was still being organised through both observation and experiment and during the 1920s and 1930s the study of child development started to grow as a movement, particularly in the USA with the founding of Institutes of Child Study or Child Welfare in university centres such as Iowa and Minnesota. Minute observations were made of young children in their developmental phase along with normal and abnormal behaviour and adjustment. In the 1920s Jean Piaget started his long and passionate career in child psychology, blending observation and experiment in his studies of children’s thinking.
The observations carried out in naturalistic settings was soon criticised by the empiricists of the behavioural movement in the 1940s and 1950s [although it continued to be the method of choice in the study of animal behaviour by zoologists]. This led to many psychologist carrying their experiments under laboratory conditions with statistical methods, and such experiments although come with some advantages from the perspective of empirical statistics, they do have limitations and drawbacks [e.g. on measuring qualitative aspects of personality such as emotions, values, etc]. It should be noted that much of the laboratory work on child development from the 1950s and 1960s has been described by Urie Bronfenbrenner (1979) as “the science of the behaviour of children in strange situations with strange adults”.
Schaffer (1996, pp. xiv – xvii) notes other changes in the methods in which psychologists now approach child development, such as the importance in understanding the processes of how children grow and develop rather than simply outcomes, and to integrate findings from a range of sources at different levels of analysis – for example meaningful others, community [geography, socio-linguistics, arts, etc] and culture [religion, nationality(ies), education, class, etc).
In the course of this essay, we will be integrating perspectives to make the most of the findings in distinguishing differences in personality, by reflecting on the links to be made by psychologists between the concept of the child’s “internal working model of relationships” and discoveries about the “theory of mind”.
It is fundamental to acknowledge that psychology itself is mostly based on accurate approximations due to the statistical methods used and the problematic nature of the qualitative variables measured, and not precision. And with this in mind, we should accept the complementary virtues of various different methods of investigation and gain a sense that the child’s process of development and the socio-behavioural context in which they exist are closely intertwined, each having an influence on the other.
Defining development according to world views
Intellectuals and researchers who study development also have different views on the topic, that is, the way in which development is defined, and the areas of development that are of interest to individual researchers generally orients them towards specific methodologies and philosophy when studying development.
We are now going to look at the 2 main views in the study of development given by psychologists who hold different views or sometimes combine elements of both, like ourselves, being firmly on the organic perspective of development and construction.
A world view [also known as paradigm, model, or world hypothesis] can be characterised as “a philosophical system of thinking, perceiving and feeling [ideas and more] that serves to organise a set or family of scientific theories and associated scientific methods” (1986, p. 42).
They are beliefs we adopt because it aligns with our values, and these are qualitative and often not open to common reductive empirical tests – that is precisely why we believe them!
Lerner and others note that many developmental theories appear to fall under one or two world views: organismic and mechanistic.
Organismic World View
The organismic world view which is the main view that we adopted to be the foundation of the Organic Theory, is one that sees a human being on earth as a biological organism that is inherently active and continually interacting with the environment [all aspects and dimensions], and therefore helping to shape its own development. The organismic worldview emphasises the interaction between maturation and experience that leads to the development of new internal, psychological structures for processing environmental input (e.g. Getsdottir & Lerner, 2008).
As Lerner states: “The Organismic model stresses the integrated structural features of the organism. If the parts making up the whole become reorganised as a consequence of the organism’s active construction of its own functioning, the structure of the organism may take on a new meaning; thus qualitatively distinct principles may be involved in human functioning at different points in life. These distinct, or new, levels of organisation are termed stages…” (p.57). A good analogy would be qualitative changes that take place when the molecules of two gasses hydrogen and oxygen, combine to form a liquid, water. Many other qualitative changes happen to water when it changes from frozen (ice) to liquid (water) to steam (vapour). Depending on the temperature, these qualitative changes in the state of water are easily reversed, BUT in human development the qualitative changes that take place are very rarely, if ever, reversible – that is, each new stage represents an advance on the previous stage, and the organism [human being] does not regress to former stages.

The main argument is that the new stage is not simply reducible to components of the previous stage; it represents new characteristics that were not present in the previous stage.
For example, the organism appears to pass through structural changes during foetal development [See Picture A].
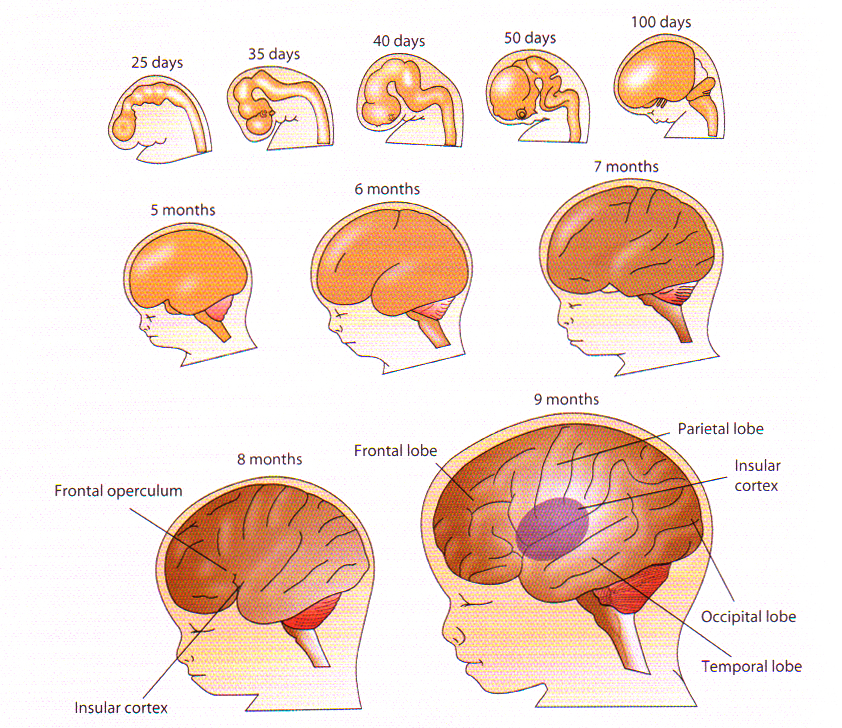
PICTURE A. Development of the human foetal brain / Source: Adapted from J.H.Martin (2003), Neuroanatomy Text and Atlas (3rd ed., p.51). Stamford, CT:Appleton & Lange.
In the initial stage [Period of the Ovum – first few weeks after conception] cells multiply and form clusters; in the second stage [Period of the Embryo – 2 – 8 weeks] the major body parts are formed by cell multiplication, specialisation and migration as well as cell death; in the last stage [Period of the Foetus] the body parts mature and begin to operate as an integrated system [e.g. head orientation towards and away from stimulation, arm extensions and grasping, thumb sucking, startles to loud noises, and so on (Fifer, 2010; Hepper, 2007)]. It is important to understand that similar stages of psychological development are postulated to happen after birth also, and the individual from one stage to another is different with new abilities that cannot be reversed.
Jean Piaget is perhaps the greatest and best example of a successful organismic theorist. Piaget suggested that cognitive development occurs in stages and that the reasoning of the child at one stage is qualitatively different from that of the earlier or later stages.

“Chaque civilisation se forge un mythe destiné à expliquer son apparition et construit sa tradition écrite autour d’un support privilégié” / Découvrez (Liens): (i) l’aventure des écritures et (ii) l’aventure du livre | Source: La Bibliothèque Nationale de France (BNF)
The main job of the developmental psychologist who believes in the organismic worldview [like ourselves] is to determine when [i.e., at what age?] different psychological stages operate and what variables and processes represent the different between stages and determine the transition between them.
Mechanistic World View
From the mechanistic world view, it is assumed that a person can be broken down into components and can be represented as being like a machine [such as a computer], which is inherently passive until stimulated by the environment [this view seems to be more in line with the early British thinkers about the brain]. Human behaviour is reducible to the operation of fundamental behavioural units [e.g. habits] that are acquired in a progressive, cumulative manner. The mechanistic view assumes that the frequency of behaviours can increase with age due to various learning processes and they can decrease with age when they no longer have any functional consequence, or lead to negative consequences [such as punishment]. The developmental psychologists job here is to study environmental factors, or principles of learning, which determine the way organisms respond to stimulation, and which results in increases, decreases, and changes in behaviour.
Quite unlike the organismic world view, the mechanistic world view sees development as reflected by a more continuous growth function, rather than occurring in qualitatively different stages, and the child is believed to be passive rather than active in shaping its own development and its environment. This mechanistic view is generally embraced by behaviourists and cognitive-behaviourists who function on a reductionist philosophy based on the limitations of the scientific method when faced with understanding psychology and the mechanism of mind; instead they tend to focus on measurable behaviour and treat the brain as an information processing centre with a highly similar logic to a computer. The mechanistic view while being fairly grotesque due to its reductionist values, has revealed to be very practical in the study of human-machine interaction and along with new cognitive methods, it has helped to enhance the design of technological equipment to improve human experience in a wide range of areas.
As for us, we are mostly on the perspective of the organismic school of thought but refuse to completely dismiss all the mechanistic world view’s elements, because some of it can be embedded as secondary cognitive processes carried out by the conscious or preconscious areas of the mind when appraising stimuli from an organism’s environment. Hence, some elements can be embedded in understanding interaction with basic objects and elements of an organism’s “external” [not internal] environment, but to fully base our thoughts and behaviour on a mechanistic world view would arguably be irrationally reductionist.
Theories of Development
“Es gibt nichts Praktischeres al seine gute Theorie.”
–Emmanuel Kant (1724 – 1804)
“There is nothing so practical as a good theory.”
-Kurt Lewin (1944, p. 195)
Human development is complex and it would be irrational to expect a single universal theory of development that could do justice to this complexity, and indeed no theory of development attempts to do so. Each theory attempts to account for only a limited range of development and it is often the case that within each area of development there are competing theoretical views, each attempting to account for the same aspects of development. We shall see below some of this complexity and conflict in our account of different theoretical views.
First of all, it would be helpful to understand what is implied by a “Theory” in the field of developmental psychology. A theory of development is a scheme or system of ideas that is generally based on evidence and attempts to explain, describe and predict behaviour and development. So, from this account, it is quite clear that a theory aims to bring order to what might otherwise be a chaotic mass of information – and hence why there may indeed not be anything more practical than a good theory.
We usually deal with at least 2 kinds of theory in every area of development, we have the minor theories [that are generally concerned with very specific and narrow areas of development such as eye movements, the origins of pointing and so on], and we have the major theories which are the ones we are primarily interested in as they attempt to explain large areas of development.
They have been divided in 3 groups for the purpose of this essay, with cognition, emotion and motivation in focus:
(I) The Theory of Cognitive Development of Jean Piaget
(II) The Theory of Attachment in Emotional Development by John Bowlby
(III) The Genetic/Psychosexual Model of Development by Sigmund Freud
__________
(I) The Theory of Cognitive Development (Jean Piaget)
The theory of cognitive development we are interested in is that of Jean Piaget who saw children as active agents in shaping their own development, and not simply blank slates who passively and unthinkingly responds to whatever the environment throws at them or treats them to [an assumption that is insulting to human intelligence, hence why we do not subscribe blindly to the passive school of thought but only consider some elements related to very basic cognitive processes].
This suggests that children’s behaviour and development is motivated largely intrinsically (internally) rather than extrinsically (externally).
For Piaget and intellectuals with a firm belief in the mind as an active entity, children learn to adapt to their environment and as a result of their cognitive adaptations they are now better able to understand their world. Adaptation is an act that all living organisms have evolved to do and as children adapt, they also gradually construct more advanced understanding [internal working models] of their worlds.
These more advanced understanding of the world reflect themselves in the appearance of new stages of development. Piaget’s theory is the best and most accomplished example of the organismic world view, and it portrays children as inherently active, continually interacting with various dimensions of their environments, in such a way as to shape their own development.
With this assumption in mind, Piaget’s theory is also often referred to the Constructivist Theory.
Piaget’s Theory of Cognitive Development (0 – 12 yrs)
Jean Piaget’s theory developed out of his early interest in observing animals in their natural environment. Piaget published his first article at the age of 10 about the description of an albino sparrow that he had observed in the park, and before the age of 18, journals had accepted several of his papers about molluscs. During his adolescent years, the young theorist developed a keen interest in philosophy, particularly “epistemology” [the branch of philosophy focused on knowledge and the acquisition of it]. However, his undergraduate studies were in the field of biology and his doctoral dissertation was once again, on molluscs.
For a short while, Piaget then worked at Bleuler’s psychiatric clinic where his interest in psychoanalysis grew. As a results, he moved to France and attended the Sorbonne university, in 1919 to study clinical psychology and also pursued his interest in philosophy. In Paris, he worked in the Binet Laboratory with Theodore Simon on the standardisation of intelligence tests. Piaget’s task was to monitor children’s correct response to test times, but instead, he became much more interested in the mistakes that children made, and developed the idea that the study of children’s errors could provide an insight into their cognitive processes.
Piaget came to realise that through the process and discipline of psychology, he had an opportunity to create links between epistemology and biology. Through the integration of the disciplines of psychology, biology and epistemology, Piaget aimed to develop a scientific approach to the understanding of knowledge – the nature of knowledge and the ways in which an organism acquires knowledge. As a man who valued richness and detail, Piaget was not at all impressed by the reductionist quantitative methods used by the empiricists of the time, however, he was influenced by the work on developmental psychology by Binet, a French psychologist who had pioneered studies of children’s thinking [his method of observing children in their natural setting was one that Piaget followed himself when he left the Binet laboratory].
Piaget later integrated his own experience of psychiatric work in Bleuler’s clinic with the observational and questioning strategies that he had learned from Binet. Out of this fusion of techniques emerged the “Clinical Interview” [an open-ended, conversational technique for eliciting children’s thinking (cognitive) processes]. It was the child’s own subjective judgement and explanation that was of interest to Piaget, as he was not testing a particular hypothesis, but rather looking for an explanation of how the child comes to understand his or her world. The method is not simple, and the team of Piaget’s researchers had to be trained for 1 year before they actually started collecting data. They were trained and educated about the “art” of asking the right questions and testing the truth of what the children said.
Piaget’s career was devoted to the quest for the mechanisms guiding biological adaptation, and also the analysis of logical thought [that derives from these adaptations and interaction with the exterior environment] (Boden, 1979). He wrote more than 50 books and hundreds of articles, correcting many of his earlier ideas in later life. At its core, the theory of Jean Piaget is concerned with the human need to discover and acquire deeper understanding and knowledge.
Piaget’s incredible output of concepts and ideas characterises his attitude towards constant construction and reconstruction of his theoretical system, which was quite consistent with his philosophy of knowledge, and perhaps indirectly to the school of thought of the mind as an “active” entity.
This section will explore the model of cognitive structure developed by Piaget along with the modifications and some of the re-interpretations that subsequent Piagetian researchers have made to the master’s initial ideas. Although many details have been questioned, it is undeniable that Piaget’s contribution to the understanding of thinking processes [cognitive] of both children and adults.
One great argument made by the theorist suggested that if we are to understand how children think we ought to look at the qualitative development of their problem-solving abilities.
Two famous examples from Piaget’s experiments will be considered that explore the thinking processes in children, showing how they develop more sophisticated problem-solving skills.
Example 1 – One of Piaget’s dialogue with a 7-year-old
Adult: Does the moon move or not?
Child: When we go, it goes.
Adult: What makes it move?
Child: We do.
Adult: How?
Child: When we walk. It goes by itself.
(Piaget, 1929, pp. 146-7)
From this example and other observations based on the similar theme, Piaget described a particular period in childhood which is marked by egocentrism. Since the moon appears to move with the child, she concluded that it does indeed do so. But as the child grows and her sense of logic follows, there is a shift from her own egocentric perspective where the child starts to learn to differentiate between what she sees and she “knows”. Gruber and Vonèche (1977) provide a good example of how an older child used her sense of logic to investigate the movement of the moon. This particular child had sent his younger brother for a walk down the garden while he himself remained immobile. The younger child reported that the moon moved with him, but the older boy realised from his observation that the moon did not move and could then disprove this wrong information with his brother.
Example 2 – Estimating the Quantity of a Liquid
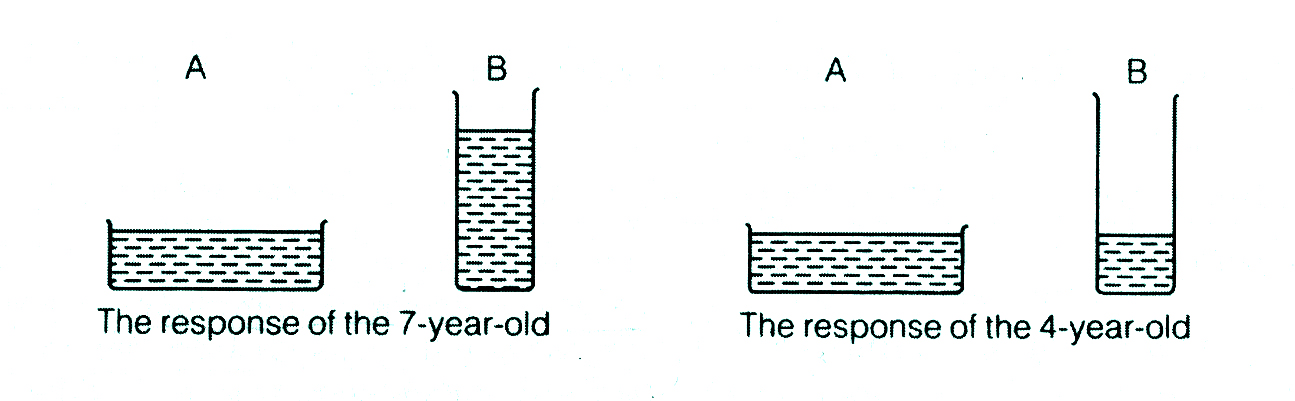
FIGURE A. Estimating a quantity of liquid
This example is taken from Piaget’s research into children’s understanding of quantity. Let us assume that John [aged 4] and Mary [aged 7] are given a problem; two glasses, A and B, are of equal capacity [volume] but glass A is short and wide and glass B is tall and narrow [See Figure A]. Glass A is filled to a particular height and the children would then be asked, separately, to pour liquid into glass B [tall and narrow] so that it would contain the same amount as glass A. Despite the striking proportional differences of the 2 containers, John could not grasp that the smaller diameter of glass B requires a higher level of liquid. To Mary, John’s response is incredibly senseless and stupid: of course one would have to add more to glass B. Piaget interestingly saw the depth of the argument that was in the responses of those children. John could not “see” that the liquid in A and the liquid in B are not equal, because his thought processes are using a mechanism that is qualitatively different in terms of reasoning and that is not yet developed [perhaps due to physiological/hardware limitations] and lacks the mental operations that would have allowed him to solve the problem. Mary, the 7 year old girl finds it hard to understand 4 year old John’s stupidity and why he could not perceive his error.
Facing this situation, Piaget brilliantly proposed that the essence of knowledge is “activity” – a line of thought and perspective adopted by many psychologists and intellectuals from the German and French school of Lacan quite opposite to the early British thoughts that assumed the mind to be “passive” and mostly shaped by the effects of the outside environment. This argument is not only one that embraces human ingenuity and creativity and acknowledges our instinctual drives to thrive and succeed but also characterises the mind as an entity with high creative power instead of simple junction of neurons conditioned to react to stimuli from its environment almost helplessly as the “passive” school assumed it to be. Hence, to Piaget and ourselves, the essence of knowledge is “activity”, he could be referring to the infant directly manipulating objects and in doing so also learning about their properties. It may also refer to a child pouring liquid from one glass to another to find out which has more in it. Or it may refer to the adolescent forming hypotheses to solve a scientific dilemma. In the examples mentioned, it is important to note that the learning process of the child is taking place through “action”, whether physical (e.g. exploring a ball of clay) or mental (e.g. thinking of various outcomes and reflecting on what they mean). Piaget’s emphasis on activity was important in stimulating the child-centred approach to education, because he firmly believed that for lasting learning to occur, children would not only have to manipulate objects but also manipulate and define ideas. The major educational implications of Piaget will be discussed later in this section.
Assumptions of Piaget’s Theory of Development: Structure & Organisation
Through his carefully devised techniques, and using observations, dialogues and small-scale experiments, Piaget suggested that children progress through a series of stages in their thinking, each of which synchronises with major changes in the structure or logic of their intelligence. [See Table A]
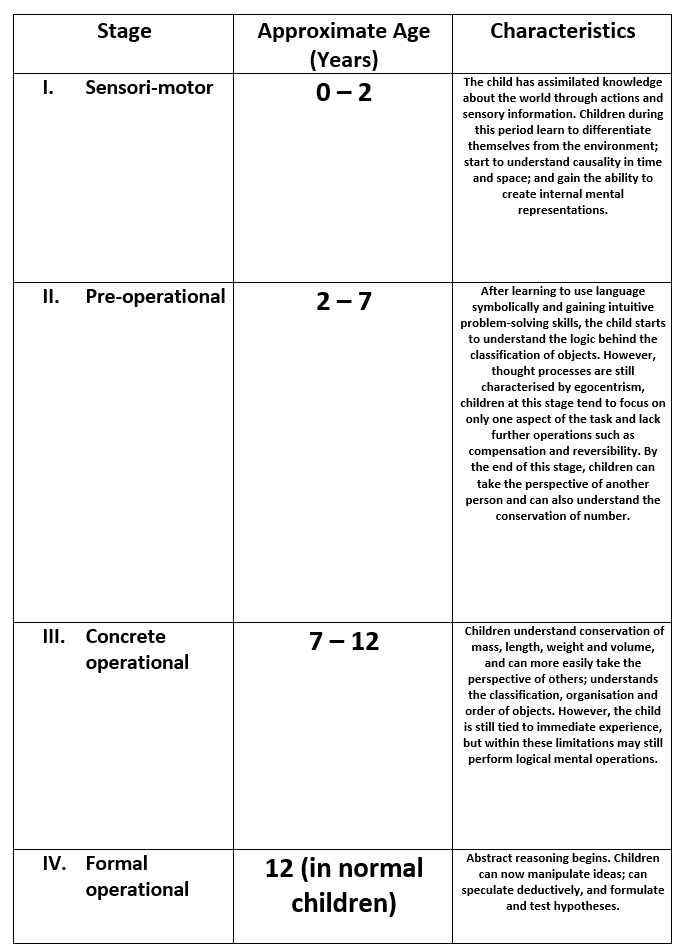
TABLE A. The Stages of Intellectual Development in Piaget’s Theory
Piaget named the main stages of development and the order in which the occurred as:
I. The Sensori-Motor Stage [0 – 2 years]
II. The Pre-Operational Stage [2 – 7 years]
III. The Concrete Operational Stage [7 – 12 years]
IV. The Formal Operational Stages [12 years but may vary from one child to the other]
Piaget’s structures are sets of mental operations, which can be applied to objects, beliefs, ideas or anything in the child’s world, and these mental operations are known as “schemas”. The schemas are characterised as being evolving structures, in other words, structures that grow and change from one stage to the next.
The details of each section of the 4 stages will be explored below, however it is fundamental that we first understand Piaget’s concept of the unchanging or “invariant” [to use his own term – this may be related to temperament but here it involves another set of abilities] aspects of thought, which refers to the broad characteristics of intelligent activity that remains constant throughout the human organism’s life.
These are the organisation of schemas and their adaptation through assimilation and accommodation.
Organisation: Piaget used this term to explain the innate ability to coordinate existing cognitive structures, or schemas, and combine them into more complex systems [e.g. a baby of 3 months old has gained the ability to combine looking and grasping, with the earlier reflex of sucking]. The baby is able to perform all three actions together when feeding from her mother’s breast or a feeding bottle, an ability that the new born child did not originally have in his/her repertoire. A further example would be Ben who at the age of 2 had learned to climb downstairs while carrying objects without dropping them, and also to open doors. This means that he could then combine all three operations to deliver newspaper to his grandmother in the basement flat. To note, each separate operation combines into a new action more complex than the sum of the parts.
The complexity of the organisation also grows as the schemas become more elaborate. Piaget described the development of a particular action schema in his son Laurent as he attempted to strike a hanging object. Initially, Laurent only made random movement towards the object, but at the age of 6 months the movements had evolved and were now deliberate, focused and well directed. As Piaget put it in his description, at 6 months old, Laurent possessed the mental structure that guided the action involved in hitting a toy. Laurent had also gained the ability to accommodate his actions to the weight, size and shape of the toy and its distance from him.
The next invariant function, “adaptation” is characterised by the striving of the organism for balance [or equilibrium] with the environment, and is achieved through the further processes of “assimilation” and “accommodation”. During the process of assimilation, the child’s repertoire of knowledge expands and he/she takes in [learns about] a new experience [and the knowledge acquired with it] and fits it into an existing schema. For example, a child may learn the words “dog” and “car”, and following this enigmatic event, the child may call all animals “dogs” [i.e. different animals taken into a schema related to the child’s understanding of dog], or all vehicles with four wheels are called “cars”. The process of accommodation balances this erroneous process, where the child adjusts an existing schema to fit in with the nature of the environment [i.e. from experience, the child begins to perceive that cats can be distinguished from dogs, and may develop schemas for these 2 different animals – also that cars can be distinguished from other vehicles such as trucks or lorries.
By these two processes, namely assimilation and accommodation, the child achieves a new state of equilibrium which is however not permanent as this balance is generally soon upset as the child assimilates further new experiences or accommodates her existing schemas to another new idea.
Equilibrium only seems to prepare the child for more disequilibrium through further learning and adaptation; these two processes occur together and cannot be thought of separately. Assimilation provides the child with consolidation for mental structures; and accommodation results in growth and change. All adaptations contains the components of both processes and striving for balance between assimilation and accommodation [Remember: Organisation Adaptation + (Assimilation & Accommodation)] leads to the child’s intrinsic motivation to learn [This is also reminiscent of the psychodynamic school of thought as several processes colliding to find balance in its model of the mental life of the individual mind]. When new experiences are within the child’s response range in terms of abilities, then conditions are said to be at their best for change and growth to occur.
The Stages of Cognitive Development
To adepts of Piaget’s outlook, intellectual development is a continuous process of assimilation and accommodation. We will not describe the four stages identified in the development of cognition from birth to about 12 years old [in normal children]. This order is similar for all children but the age these milestones are achieved may vary from one child to another – with the stages being:
I. The Sensori-Motor Stage [0 – 2 years]
II. The Pre-Operational Stage [2 – 7 years]
III. The Concrete Operational Stage [7 – 12 years]
IV. The Formal Operational Stages [12 years but may vary from one child to the other]
I. The Sensori-Motor Stage (about 0 – 2 years) | Stage 1 of 4
During the sensori-motor stage the child changes from a newborn, who focuses almost entirely on immediate sensory and motor experiences, to a toddler who possesses a rudimentary capacity for thinking. Piaget described in detail the process by which this occurs, by documenting his own children’s behaviour. On the basis of such observations, carried over the first 2 years of life, Piaget divided the sensori-motor stage into 6 sub-stages. [See Table B]
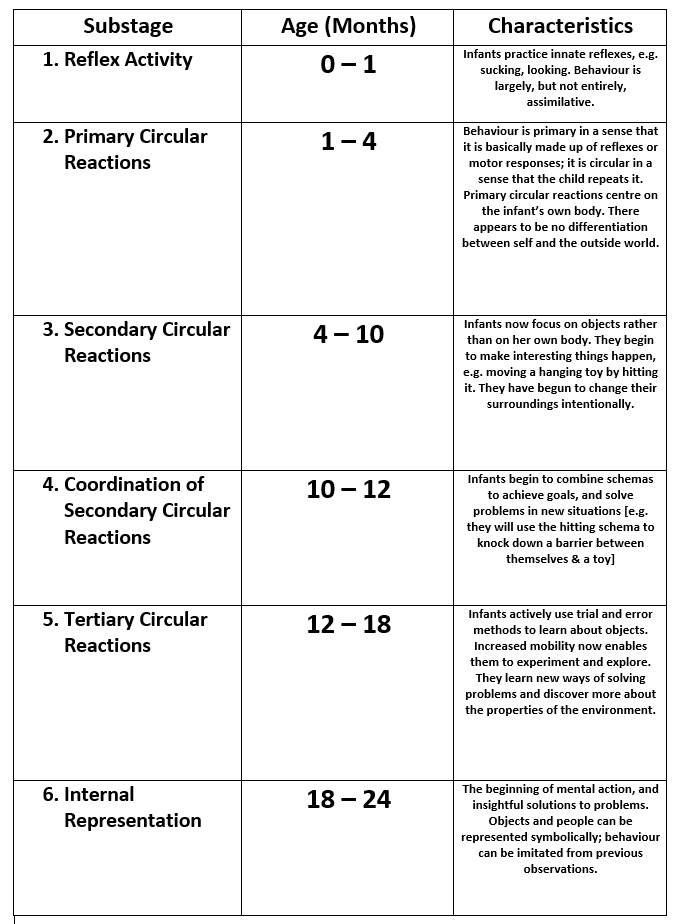
TABLE B. Substages of the sensori-motor period according to Piaget
The first substage, reflex activity, included the reflexive behaviours and spontaneous rhythmic activity with which the infant is born. Piaget called the second substage primary circular reactions. He used the term “circular” to emphasise how children tend to repeat an activity, especially those that are pleasing or satisfying (e.g. thumb sucking). The term “primary” refers to simple behaviours that are derived from the reflexes of the first period [e.g. thumb sucking develops as the thumb is assimilated into a schema based on the innate suckling reflex].
Secondary circular reactions refer to the child’s willingness to repeat actions, but the word “secondary” is used here to point out the behaviours that are the child’s very own. In other words, she is not limited to just repeating actions based on early reflexes, but having initiated new actions, she can now repeat these if they are satisfying. However, at the same time, these actions tend to be directed outside the child (unlike simple actions like thumb sucking) and are aimed at influencing the environment around her.
This is Piaget’s description of his own daughter Jacqueline at 5 months old, kicking her legs (in itself a primary circular reaction) in what gradually ascends to a secondary circular reaction as the leg movement is repeated not just for itself, but is initiated in the presence of a doll.
Jacqueline looks at a doll attached to a string which is stretched from the hood to the handle of the cradle. The doll is approximately the same level as the child’s feet. Jacqueline moves her feet and finally strikes the doll, whose movement she immediately notices… The activity of the feet grows increasingly regular whereas Jacqueline’s eyes are fixed on the doll. Moreover, when I remove the doll Jacqueline occupies herself quite differently; when I replace it, after a moment, she immediately starts to move her legs again.
(Piaget, 1936, p. 182)
In displaying such behaviours, Jacqueline seemed to have established a general relation between her movement and the doll’s, and was also engaged in a secondary circular reaction.
Coordination of Secondary Circular Reactions, being substage 4 of the Sensori-motor period, and as the word “coordination” implies, it is particularly at this substage that children begin to combine different behavioural schema. In the following extracted section, Piaget described how his daughter (aged 8 months) combined several schemas, such as “sucking an object” and “grasping an object” in a series of coordinated actions when playing with a new object:
Jacqueline grasps an unfamiliar cigarette case which I present to her. At first she examines it very attentively, turns it over, then holds it in both hands while making the sound apff (a kind of hiss which she usually makes in the presence of people). After than she rubs it against the wicker of her cradle then draws herself up while looking at it, then swings it above her and finally puts it in her mouth.
(Piaget, 1936, p. 284)
Jacqueline’s behaviour illustrates how a new object is assimilated to various existing schema in the fourth substage. In the following stage, that of tertiary circular reactions children’s behaviours become more flexible and when they repeat actions they may do so with variations, which can lead to new results. By repeating actions with variations, children are, in effect, accommodating established schema to new contexts and needs.
The final sub-stage of the sensori-motor period is known as the substage of Internal Representations and it refers to the child’s achievement of mental representation. The previous substages the child has interacted with the world through her physical motor schema, another way of phrasing it would be that, she has acted directly on the world. In this final substage, she can now act “indirectly” on the world because she has developed the capacity to hold mental representations of the world – that is, she can now think and plan.
As evidence for children attaining the level of mental representation, Piaget pointed out that by this substage children have a full concept of object permanence. Piaget noticed that very young infants ignored even highly attractive objects once they were out of sight [e.g. a child reaching for a toy, but then the toy is suddenly covered with a cloth and it immediately leads to the child losing all interest in it and would not attempt to search for it, and might even just look away]. According to Piaget it was only after the later substages that children demonstrated an awareness [by searching and trying to retrieve the object] that the object was “permanently” present even if it was temporarily out of sight. Searching for an object that cannot be seen directly implies that the child has a memory of the object, i.e. a mental representation of it.
It is only towards the end of the sensori-motor period that children demonstrated novel patterns of behaviour in response to a problem. For example, if a child wants to reach for a toy and comes across an object between herself and the desired toy, younger children might just try and reach for the toy directly and it is possible that the child knocks over the object while reaching for the target toy – this is best described as “Trial and Error” performance. In the later substages, the child might solve the problem by instead first removing the object out of the way before reaching for the desired toy. Such structured behaviour suggests that the child was able to plan ahead, which indicates that he/she had a mental representation of what she was going to do.
An example of planned behaviour by Jacqueline was given where she was trying to solve the problem of opening a door while carrying two blades of grass at the same time:
She stretches out her right hand towards the knob but sees that she is cannot turn it without letting go of the grass. She puts the grass on the floor, opens the door, picks up the grass again and enters. But when she wants to leave the room things become complicated. She put the grass on the floor and grasps the door knob but then she realises that in pulling the door towards her she will simultaneously chase away the grass which she placed between the door and the threshold. She therefore picks it up in order to put it outside of the door’s zone of movement.
(Piaget, 1936, pp. 376-7)
Jacqueline solved the problem of the grass and the door before she opened the door. It is assumed that she would have had a mental representation of the problem, which permitted her to work out the solution, before she acted.
A third line of evidence for mental representations comes from Piaget’s observation of deferred imitation, that is when children carry out a behaviour that is a reflection of copied behaviour that was previously taken in by the developing child. Piaget provides a good example of this:
At 16 months old Jacqueline had a visit from a little boy of 18 months who she used to see from time to time, and who, in the course of the afternoon got into a terrible temper. He screamed and he tried to get out of a playpen and pushed it backward, stamping his feet. Jacqueline stood observing him in amazement, having never witnessed such a scene before. The following day, she herself screamed in her playpen and tried to move it, stamping her foot lightly several times in succession.
(Piaget, 1951, p. 63)
This suggests that if the little boy’s behaviour was repeated by Jacqueline a day later, she would have had to have retained an image of his behaviour, i.e. she had a mental representation of what she had seen from the day before, and that representation provided the basis for her own copy of the temper tantrum.
To conclude, during the sensori-motor period, the child advances from very simple and limited reflex behaviours at birth, to complex behaviours at the end of the period. The more complex behaviours depend on the progressive combination and elaboration of the schema, but are, at the beginning, limited to direct interactions with the world – thus, the name Piaget gave to this period because he thought of the child developing through her sensori-motor interaction with the environment. It is only towards the end of that period that the child is not limited to immediate interaction anymore because she has now developed the ability to mentally represent her world [mental representation], and with this ability the child can manipulate her mental images (or symbols) of her world, in other words, she can now act on her thoughts about the world as well as on the world itself.

Revisions of the Sensori-motor Stage
Jean Piaget’s observations of babies during this first stage lasting until 2 years of age, have been largely confirmed by subsequent reseachers, however Piaget may have underestimated children’s mental capacity to organize the sensory and motor information they take in. Several investigators have shown that children have abilities and concepts earlier than Piaget thought.
Bower (1982) examined Piaget’s hypothesis that young children did not have an appreciation of objects if they were not in sight. For this experiment, children a few months old were recruited and shown an object, and shortly after a screen was moved across in front of the object [so that it would be hidden/unseen from the child’s visual field], to then finally be moved back to its original position. This scenario was presented with 2 slight changes: in Condition 1 the object was still in place and hence seen again by the child when the screen was moved back to its original location; and in Condition 2, the object was removed so the child would perceive the object to have disappeared when the screen was moved back. After monitoring the children’s heart rate to measure changes [which reflect surprise]. To go back to Piaget’s assumptions from his qualitative observations, it would be assumed that children of a few months old do not retain information about objects that are no longer present, and if this was the case, we would not register any heart rate change because as there should be no element of surprise [i.e. the child would not expect an object to be there once the screen was moved back to its original location], thus in Condition 2, no reaction should be displayed by the children, however it was found that children displayed more surprise in Condition 2 and Bower inferred that the children would have had an expectation of the object to still be in its position or “re-appear” after the screen was moved back – this would be the evidence that young children must retain a mental representation of the object in their mind [could be interpreted as young children having some basic form of object permanence even if not properly developed at an earlier age than the assumptions of Piaget based on the results of his experimental methods].
In a further experiment, Baillargeon and DeVos (1991) showed 3-month-old children objects that moved behind a screen and then re-appeared from the other side of the screen. The upper half of the screen had a window and in one condition the children saw a short object move behind the screen [the object was small and below the level of the window and hence when it passed behind the screen it was completely out of sight / not visible, until it appeared at the other side of the screen].
In a second condition a taller object was passed behind the screen, and it was high enough to be seen through the window as it passed from one side to the other. Furthermore, Baillargeon and DeVos created an “impossible event” by passing the tall object through the screen without it appearing through the window, and it lead to the children displaying more interest by looking longer at the scenario than that with the small object. This lead to the argument that children reacted so, due to their expectation of the taller object to appear through the window, and hence this would suggest that young children early in the sensori-motor stage have an awareness of the continued existence of objects even when they are out of view. These results along with that of Bower (1982) seem to suggest that young children to have “some” understanding of object permanence earlier than assumed.
Another one of Piaget’s conclusion was also investigated further by another group of researchers who wanted to find out if children only developed planned action [which demonstrated their ability to form mental representations] at the end of the sensori-motor stage. Willatts (1989) placed an attractive toy on a cloth, out of the reach of 9-month-old children; the children could pull the cloth to access the attractive toy. However, the children could not reach the cloth directly since it was not accessible as Willatts placed a light barrier between the child and the cloth [the child had to move the barrier to reach the cloth]. The experiment showed that children were able to access the toy by carrying out appropriate the series of actions [i.e. first moving the barrier, then pulling the cloth to bring the toy within reach]. Most importantly, many of the children carried out the correct actions within the first occasion of being presented with the problem without the need of going through a “trial and error” phase. Willatts argued that for such young children to demonstrate novel planned actions, it may be inferred from such behaviour that they are operating on a mental representation of the world which they can make use of to organise their behaviour before carrying it out [This is also earlier than assumed by Piaget’s experiments].
Another point made by Piaget was that deferred imitation was an evidence that children should have a memory representation of what they had seen earlier. Soon after birth however it was found that babies are able to imitate the facial expression of an adult or the head movement (Meltzoff and Moore, 1983, 1989), however such imitation is performed in the presence of the stimulus being imitated. From Piaget’s experiments, it was initially deduced that stored representations are only achieved by children towards the end of the sensori-motor stage, however, Meltzoff and Moore (1994) showed that 6-week old infants could imitate a behaviour a day after they had seen the original behaviour. In Meltzoff and Moore’s study some children saw an adult make a facial gesture [e.g. sticking out her tongue] and others just saw the adult’s face while she maintained a neutral expression. The next day, all the children in the experiment saw the same adult, however this time, she kept a passive face. Compared to the children who had not seen any gesture, the children who had seen the tongue protrusion gesture the day before were more likely to make tongue protrusions to the adult the second time they saw her. Meltzoff and Moore argued that for the children to be able to perform those actions they would have had to have a mental representation of the action at a much earlier age than Piaget’s experiments concluded
II. The Pre-operational Stage (about 2 – 7 years) | Stage 2 of 4
This stage will be divided in 2 periods: (a) The Pre-conceptual Period (2 – 4 years) and (b) the Intuitive Period (4 – 7 years)
(a) The Pre-Conceptual Period (2 – 4 years)
The pre-conceptual period builds on the ability for internal, or symbolic thought to develop based on the latest advancements during the final stages of the sensori-motor period. During the pre-conceptual period [2 – 4 years old], we can observe a rapid increase in children’s language which, in Piaget’s view, results from the development of symbolic thought. Piaget unlike other theorists of language [who suggested that thought emerges from linguistic competence] argued that thought arises out of action and this idea is supported by research into cognitive abilities of deaf children who, despite limitations in language, have the abilities for reasoning and problem solving. Piaget argued that thought shapes language far more than language shapes thought [at least during the pre-conceptual period], and symbolic thought is also expressed in imaginative play.
However there are some limitations in the child’s abilities at the pre-conceptual period (2-4 years) of the pre-operational stage. The pre-operational child is still centred in her own perspective and finds it difficult to understand that other people can look at things differently. Piaget called this the “self-centred” view of the world and used the term egocentrism.
Egocentric thinking occurs due to the child’s belief that the universe is centred on herself, and thus finds it hard to “decentre”, that is, to take the perspective of another individual. The dialogue below gives an example of a 3-year-old’s difficulty in taking the perspective of another person:
Adult: Have you any brothers or sisters?
John: Yes, a brother.
Adult: What is his name?
John: Sammy.
Adult: Does Sammy have a brother?
John: No.
It is quite clear here that 3-year old John’s inability to decentre makes it hard for the child to realise that from Sammy’s perspective, he himself is a brother.
The egocentric trait at this particular period of development is apparent in their flawed perspective taking tasks. One of the most famous experiments carried out by Piaget is the three mountains experiment tasks, and it involves exploring children’s ability to see things from the perspective of another. In 1956, Piaget and Inhelder asked children between the ages of four and twelve [4 – 12 years old] to say how a doll would perceive an array of three mountains from different perspectives [i.e. by placing the doll at different locations].
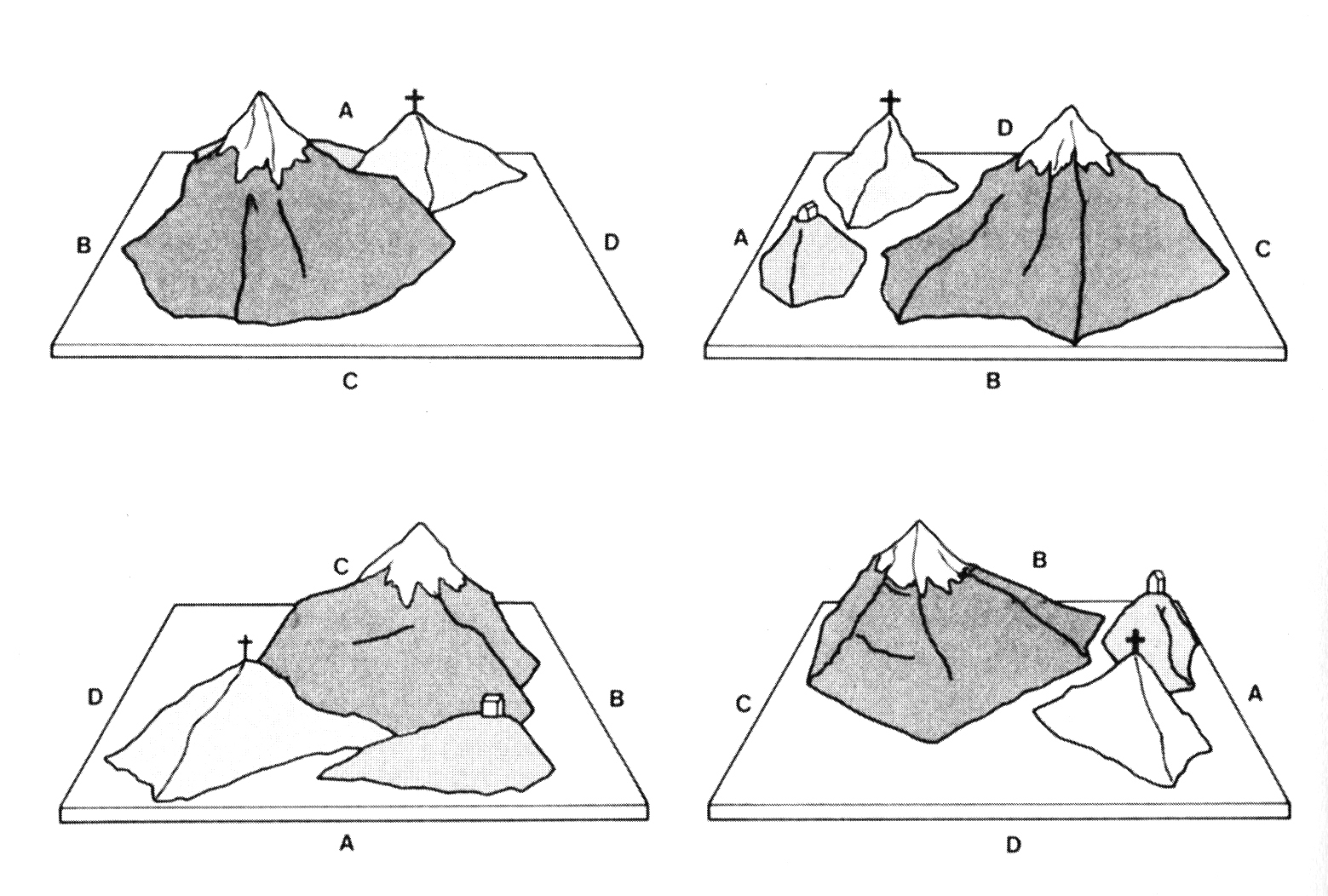
FIGURE J. Model of the mountain range used by Piaget and Inhelder viewed from 4 different sides
For example in Figure J, a child might be asked to sit at position A, and a doll would be placed at one of the other positions (B, C or D), then the child would be made to choose from a set of different views of the model, the view that the doll could see. When four and five year old children [4 and 5 years old] were asked to do this task, they often chose the view that they themselves could see (rather than the doll’s view) and it was not until 8 or 9 years of age that children could confidently work out the doll’s view. Piaget argued that this should be convincing in asserting that young children were still learning to manage their egocentricity and could not decentre from their own perspective to work out the perspective / view of the doll.
However, several criticisms have been made regarding the 3 mountain tasks, and one researcher, Donaldson (1978) pointed out that the tasks were unusual to use with young children who might not have a good familiarity with model mountains or be used to working out other people’s views of landscapes. Borke (1975) carried out a similar task to Piaget, but instead of using model mountains, he used the layout of toys that young children typically spend time with in play. She also altered the way that children were asked to respond to the question about what a different person’s view would be, and found that children as young as 3 or 4 years of age had some basic understanding of how another person’s perspective would be different from another position. This was much earlier than previously deduced from Piaget’s experiments, and shows that the type of objects and procedures used in a task can have a huge impact on the performance of the children. By using mountains, Piaget may have selected a far too complex content for such young children’s perspective-taking abilities to be demonstrated optimally.
Borke’s Experiment: Piaget’s Mountains Revised & Changes in the Egocentric Landscape
Borke’s main inquisition was about the appropriateness of Piaget’s three mountain tasks for such young children, and was concerned with the aspects of the task that were not related to perspective-taking and whether this might have adversely affected the children’s performance. These aspects were:
(i) the mountain from a different angle or not may not have sparked any interest or motivation in the children
(ii) the pictures of the doll’s views that Piaget had asked the children to select may have been too taxing for their intelligence
(iii) due to the task being unusual in nature, children may have performed poorly because they were unfamiliar with such a task
Borke considered if some initial practice and familiarity with the task would improve the children’s performance, and with those points in mind, Borke repeated the basic design of Piaget and Inhelder’s experiment but changed the content of the task, avoided the use of pictures and gave children some initial practice. She also used 4 three-dimensional displays: there were a practice display and three experimental displays [see FIGURE B].
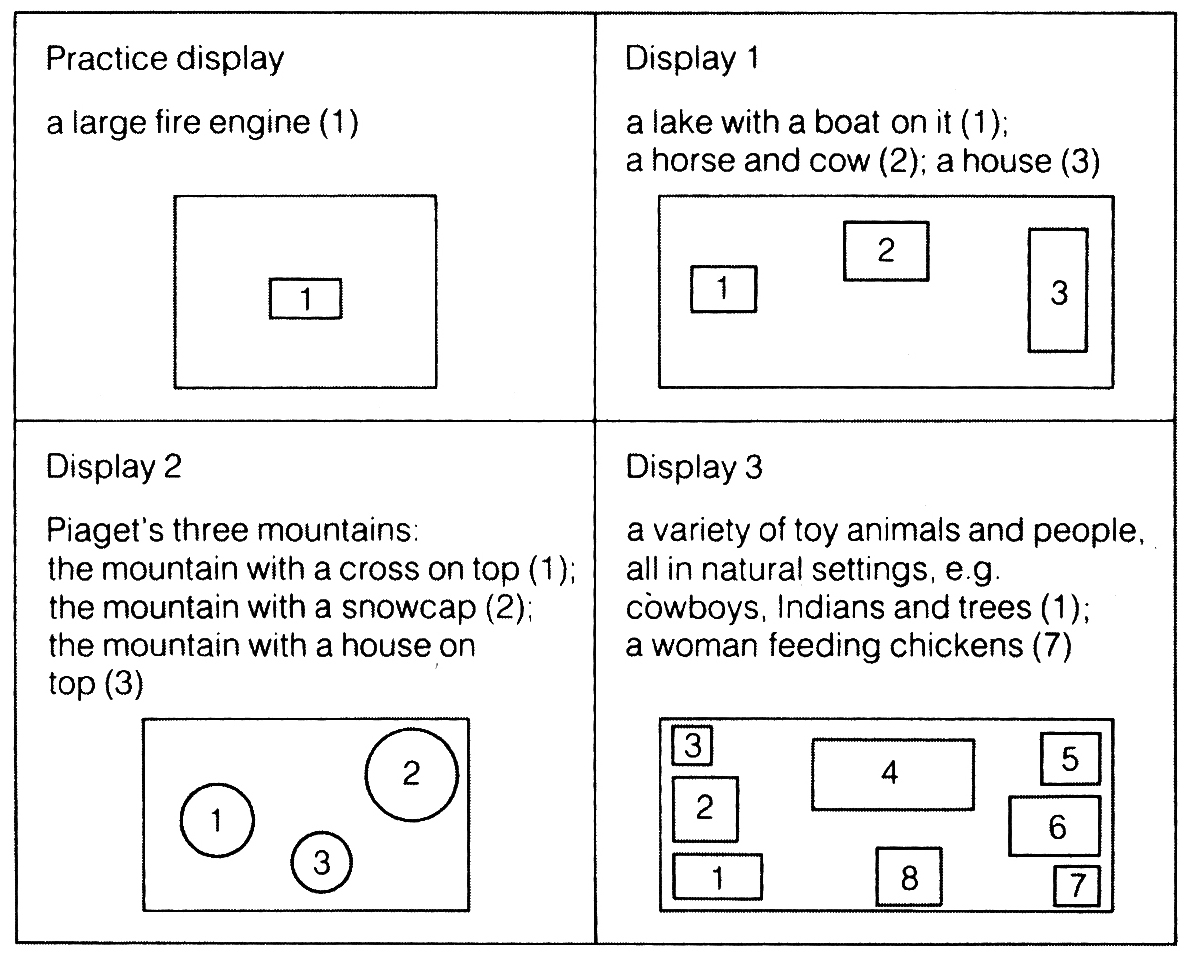
FIGURE B. A schematic view of Borke’s four three-dimensional displays viewed from above.
Borke’s participants were 8 three-year-old children and 14 four-year-old children attending a day nursery. Grover, a character from the popular children’s television show, “Sesame Street” was used for the experiment as a substitute for Piaget’s doll. There we 2 identical versions of each display (A and B), and Display A was for Grover and the child to look at, and Display B was on a turntable next to the child.
The children were tested individually and were first shown a practice display which consisted of a large toy fire engine. Borke placed Grover at one of the sides of the practice Display A so that Grover could view the fire engine from a point of view [perspective] that was different from the child’s own view of this display.
A duplicate of the fire engine [practice Display B] appeared on a revolving turntable, and Borke briefed the children, explaining that the table could be turned so that the child could look at the fire engine from ANY side. Children were then prompted to turn the table until their view of the Display B matched the exact perspective that Grover had while looking at Display A. If necessary, Borke even helped the children to move the turntable to the correct position or walked the children round Display A to show them the exact view [perspective] that Grover had in view
Once the practice session was over, the child was ready to take part in the experiment itself. This time, the procedures were similar, except no help was provided by the experimenter. Every single child was shown three dimensional displays, one at a time [see FIGURE B].
Display 1 included a toy house, lake and animals
Display 2 was based in Piaget’s model of three mountains
Display 3 included several scenes with figures and animals
Note: There were 2 identical copies of each display, and of course, children had to rotate the second copy which was on a turntable to match the perspective [view] that Grover had in sight [as prepared in the practice session].
What Borke found was that most of the children in the experiment were able to work out Grover’s perspective for Display 1 [three and four-year-olds were correct in 80% of trials] and for Display 3 [three-year-olds were correct in 79% of trials and four-year-olds, in 93% of trials. However, for Display 2 [Piaget’s mountains], the three-year-olds were correct in only 42% of trials and four-year-olds in 67% of trials. Borke calculated an analysis of variance, and found that the difference between Displays 1 & 3 and Display 2 was significant at p < 0.001. As for errors, there were no significant differences in the children’s responses for any of the 3 positions – 31% of errors were egocentric [i.e. child rotated Display B to show their OWN view/perspective of Display A, rather than Grover’s view].
Borke successfully demonstrated that the task had a major influence on the perspective-taking performances of young children. When the display included toys that the children were familiar with and hence recognisable, and when the response involved rotating a turntable to work out Grover’s perspective, even the comparatively complex Display 3 task was successfully achieved by the children.
This seems to suggest that the poor performance by the children in Piaget’s original experiment involving three mountains was due in part to the unfamiliar nature of the objects that the children were shown.
Borke concluded that the potential for understanding the viewpoint of another was already present in children as young as 3 and 4 years of age, and this seems to be a reliable addition and revision to Piaget’s original assumption that children of this age are egocentric and incapable to taking the viewpoint of others. It now seems clear that although their perspective taking abilities may not be fully developed, they tend to make egocentric responses when they misunderstood the task, but when given the appropriate conditions, they show that they are capable of working out another’s viewpoint.
However, on a final note, it is important to also consider that Borke’s finding that children as young as three years can perform correctly in perspective-taking tasks stands in firm contrast to other researchers who have found that three-year-olds have difficulty realising another person’s perspective when the child and the other person are both looking at the same picture from different point of view [e.g. at the Louvres museum] (e.g., Masangkay et al, 1974).
(a) The Pre-Conceptual Period (2 – 4 years)… continued from above
Piaget use the three mountains task to investigate visual perspective taking and it was on the basis of this task that he concluded that young children were egocentric. There are also a variety of other perspective taking scenarios, and these include the ability to empathise with other people’s emotions, and the ability to know what other people are or may be thinking depending on the scene, setting and scenario (Wimmer and Perner, 1983). In other words, young children are less egocentric than Piaget initially assumed.
(b) The Intuitive Period (4 – 7 years)
At about the age of four, there is a further shift in thinking where the child begins to develop the mental operation of ordering, classifying and quantifying in a more systematic way. The term “intuitive” was particularly chosen by Piaget because the child is largely unaware of the principles that underlie the operations she completes and cannot explain why she has done them, nor can she carry them out in a fully satisfactory way, although she is able to carry out such operations involving ordering, classifying and quantifying.

Difficulties can be observed if a pre-operational child is asked to arrange sticks in a particular order. 10 sticks of different sizes from A (the shortest) to J (the longest), arranged randomly on a table were given to the children. The child was asked to arrange them in ascending order [order of length]. Some pre-operational children could not complete the task at all. Some other children arrange a few sticks correctly, but could not complete the task properly. And some put all the smaller ones in one and all the longer one in another. A more advance response was to arrange the sticks so that tops of the sticks when order even though the bottoms were not [See FIGURE C].
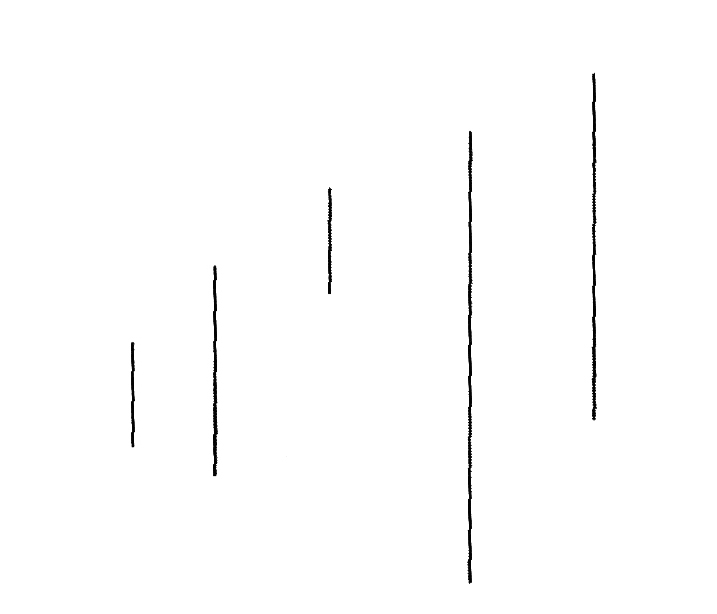
FIGURE C. The pre-operational child’s ordering of different-sized sticks. An arrangement in which the child has solved the problem of seriation by ignoring the length of the sticks.
To sum up, the pre-operational child is not capable of arranging more than a very few objects in the appropriate order.
It was also discovered that pre-operational children also have difficulty with class inclusion tasks – those that involve part-whole relations. Let us assume that a child is given a box that contains 18 brown beads and 2 white beads; all the beads are wooden. When asked “Are there more brown beads than wooden beads?” [note that the question does not make sense since all the beads are made of wood but some are brown and some are white], the pre-operational child tends to say that there are “more brown beads”. The child at the intuitive-period of the pre-operational stage finds it hard to consider the class of “all beads” [wooden] and at the same time considering the subset of beads, the class of “brown beads”[wooden + brown].
This findings is generally true for all children in the pre-operational stage, irrespective of their cultural background. Investigators further found that Thai and Malaysian children gave responses that were very similar to those of Swiss children at this stage of life [4 – 7 years old] and in the same sequence od development [the intuitive period].
Here, a Thai boy who was shown a bunch of 7 roses and 2 lotus [all are in the class of flowers], states that there are more roses than flowers [problem with class of all flowers] when prompted by the standard Piagetian questions:
Child: More roses.
Experimenter: More than what?
Child: More than flowers.
Experimenter: What are the flowers?
Child: Roses.
Experimenter: Are there any others?
Child: There are.
Experimenter: What?
Child: Lotus
Experimenter: So in this bunch which is more roses or flowers?
Child: More roses.
(Ginsburg and Opper, 1979, pp. 130-1)
One of the most extensively investigated aspects of the pre-operational child’s thinking processes is what Piaget called “conservation”. Conservation refers to the understanding that superficial changes in the appearance of a quantity do not mean that there has been any real change in the quantity. For example, if we had 10 dolls placed in line, and then they were re-arranged in a circle, it would not mean that the quantity has been altered [i.e. if nothing is added or subtracted from a quantity then it remains the same – conservation].
Piaget’s experiments revealed that children in the pre-operational stage generally find it hard to grasp the concept that an object’s qualities remain intact even if it is changed in shape and appearance. A series of conservation tasks were used in the investigations and examples are given in FIGURE D and PLATE A.
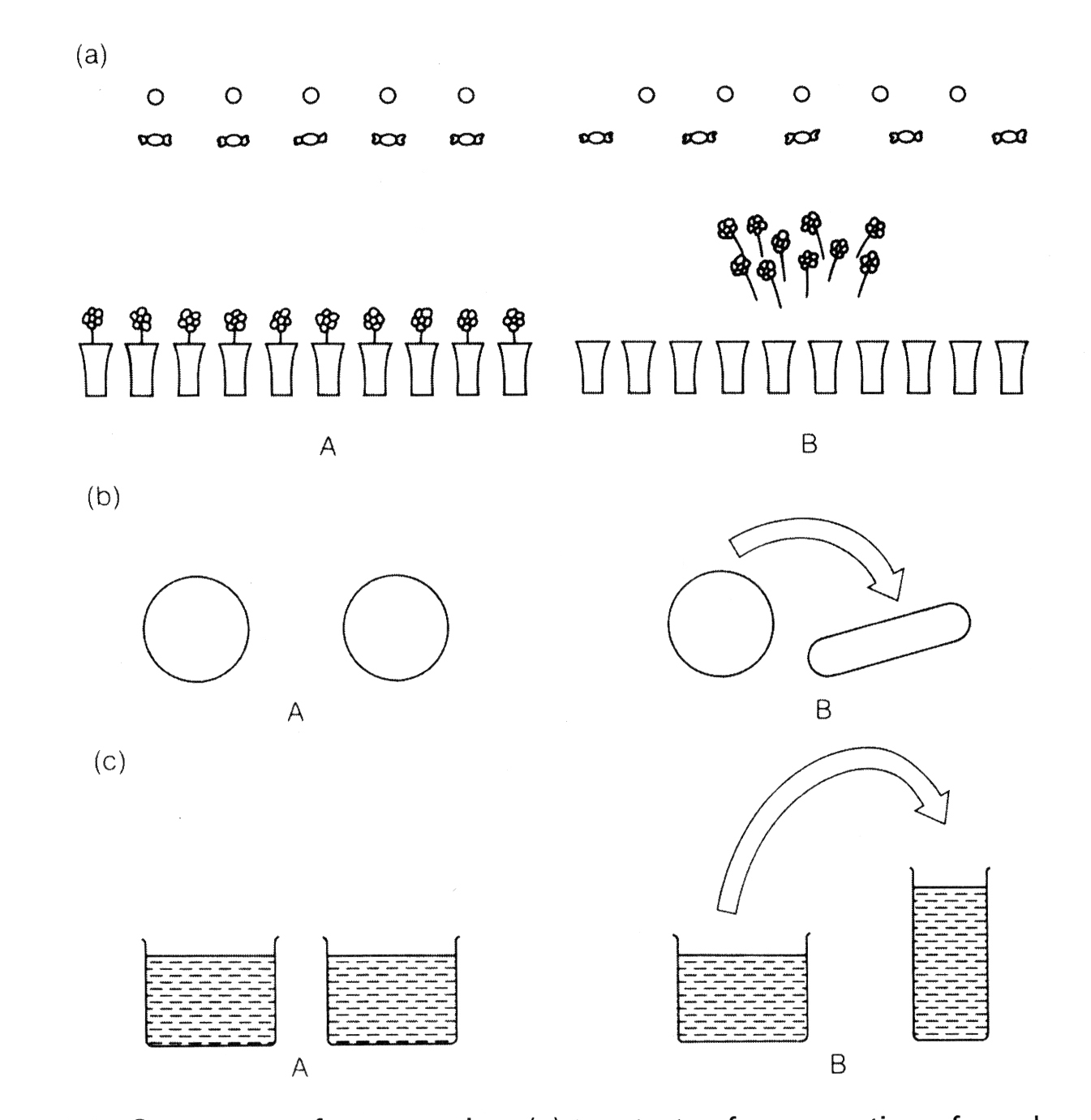
FIGURE D. Some tests of conservation: (a) two tests of conservation of number (rows of sweets and coins; and flowers in vases); (b) conservation of mass (two balls of clay); (c) conservation of quantity (liquid in glasses). In each case illustration A shows the material when the child is first asked if the two items or sets of items are the same and illustration B shows the way that one item or set of items is transformed before the child is asked a second time if they are still similar.

PLATE A. A 4-year-old puzzles over Piaget’s conservation of number experiments; he says that the rows are equal in number in arrangement (a), but not in arrangement (b) “because they’re all bunched together here”.
If 2 perfectly identical balls of clay are given to a child and if questioned about whether the quantity of clay being similar in both balls, the child will generally agree that it is. However, if one of the balls of clay is rolled and shaped into a sausage [see FIGURE D(b)], and the child is questioned again about whether the amount are similar, he/she is more likely to say that one is larger than the other. When asked about the reasons for the answer, they are generally unable to give an explanation, but simply say “because it is larger”.
Piaget suggested that a child has difficulty in a task such as this because she could only focus on one attribute at a time [e.g. if length is being focussed on, then she may think that the sausage shaped clay, being longer, has more clay it it. According to Piaget, for a child to appreciate that the sausage of clay has the same amount of clay as the ball would require an understanding that the greater length of the sausage is compensated for by the smaller cross section of the sausage. Piaget said that pre-operational children cannot apply principles such as compensation.
A further example to demonstrate this weakness in the child’s reasoning about conservation is through the sweets task [see FIGURE D(a)]. In this scenario, a child is shown 2 rows of sweets with a similar number of sweets in each row [presented with one to one layout] and when asked if the numbers match in each row, she will usually agree. Shortly after, one row of sweets is made longer by spreading them out, and the child is once again asked whether the number of sweets in similar in each row; the pre-operational child usually makes a choice between the rows suggesting that one has more sweets in it. He/she may for example think that the longer row means more objects [logic of the pre-operational child]. At this stage, the child does not realise that the greater length of the row of sweets is compensated for by the greater distance between the sweets.
Compensation is only one of several processes that can help children overcome changes in appearance; another process is known as “reversibility”. This is where the children could think of literally “reversing” the change; for example if the children imagine the sausage of clay being rolled back and reshaped into a ball of clay, or the row of sweets being pushed back together, they may realise that once the change has been reversed the quantity of an object or the number of items in the row remains similar to before. Pre-operational children lack the thought processes needed to apply principles like “compensation” and “reversibility”, and therefore they have difficulty in conservation tasks.
In the next stage, which is the third stage of development known as the “Concrete Operational Stage”, children will have achieved the necessary logical thought processes that give them the ability to use the required principles and handle conservation techniques and other problem-solving tasks easily.
Revisions of the Pre-Operational Stage
While Piaget claimed that the pre-operational child cannot cope with tasks like part-whole relations or conservations, because they lack the logical thought processes to apply principles like compensation. Other researchers have pointed out that children’s lack of success in some tasks may be due to factors other than ones associated with logical processes.
The pre-operational child seems to lack the ability to grasp the concept of the relationship between the whole and the part in class inclusion tasks, and will happily state that there are more brown beads than wooden beads in a box of brown and white wooden beads “because there are only two white ones”. Some other researchers have focussed their attention on the questions that children are asked during such studies and found them to be unusual [e.g. it is not often in every day conversation that we ask questions such as “Are there more brown beads or more wooden beads?”]
Minor variations in the wording of the questions that enhances and clarifies meaning can have positive effects on the child’s performance. McGarrigle (quoted Donaldson, 1978) showed children 4 toy cows, 3 black and 1 white, all were lying asleep on their sides. If the children were asked “Are there more black cows or more cows?” [as in a standard Piagetian experiment with a meaningless trap wording of the question] they tended not to answer correctly. McGarrigle found that in a group of children aged 6 years old, 25% answered the standard Piagetian question correctly, and when it was rephrased, 48% of the children answered correctly – a significant increase. From such an observation it was deduced that some of the difficulty of the task was in the wording of the question rather than just an inability to understand part-whole relations.
Donaldson (1978) put forward a different reason from Piaget as a cause for children’s poor performance in conservation tasks, he argued that children have a build in model of the world by formulating hypotheses that help them anticipate future events based on their past experiences. Hence, in the case of the child there is an expectation about any situation, and his/her interpretation of the words she hears will be influenced by the expectations she brings to the situation. When in a conservation experiment, for example, the experimenter asks a child if there are the same number of sweets in two rows [FIGURE D(a)]. Then one of the rows is changed by the experimenter while emphasising that it is being altered. Donaldson suggested that it is quite fair to assume that a child may be compelled to deduce that there would be a link between the change that occurred [the display change] and the following question [about the number of sweets in each row]; otherwise why would such a precise question come from an adult if there had not been any change? If the child is of the belief that adults only carry actions when they desire a change, then he/she might assume that a change has occurred.
McGarrigle and Donaldson (1974) explored this idea in an experiment with a character known as “Naughty Teddy”, and it was this character rather than the experimenter who changed the display layout and the modification was explained to the children as an “accident” [in such a context the child might have less expectation that a deliberate treatment had been applied to the objects, and there would be no reason to believe a change had taken place]. This procedure was setup in such a way because McGarrigle and Donaldson found that children were more likely to give the correct answer [that the objects remained the same after being messed up by Naughty Teddy] in this new context than in the classical Piagetian context.
Piaget was correct to point out the problems that pre-operational children face with conservation and other reasoning tasks. However, other researchers since Piaget have found out that, given the appropriate wording and context, young children seem capable of demonstrating at least some of the abilities that Piaget thought only developed later [even if these abilities are not well developed at such a stage].
Piaget also found that pre-operational children had difficulties when faced with tasks requiring “transitive inferences”. In this case, the children were showed 2 rods, A and B. Rod A was longer than Rod B, and then Rod A was taken out of sight of the children, who were then showed only Rod B and Rod C [B was longer than C]. When the children were then asked which rod was longer, Rod A or Rod C? Young children on the pre-operational stage find such questions hard and Piaget provided the explanation that these children cannot make logical inferences such as: if A is longer than B and B is longer than C, then A must be longer than C.
Bryant and Trabasso (1971) also considered transitive inference tasks and wondered whether children’s difficulties had more to do with remembering all the specific information about the objects rather than making an inference [i.e. for children to respond correctly they would not only have to make an inference but also remember the lengths of all the rods they had seen]. Bryant and Trabasso proposed that it was possible that young children [with brains still growing and developing physiologically] who have limited working memory capacity, were unable to retain in memory all the information they needed for the task.
In another scenario, children were faced with the similar task in an investigation of transitive inferences, however this time they were trained to remember the lengths of the rods [they were trained on the comparisons they needed to remember, i.e., that A was longer than B, and B was longer than C]. It is only when Bryant and Trabasson were satisfied that the children could remember all the information were they asked the test question [i.e. which rod was longer? A or C?]. The experimenters found that children could now answer correctly. So, the difficulty that Piaget noted in those tasks was more to do with forgetting some of the information needed to make the necessary comparisons, rather than a failure in making logical inferences.
III. The Concrete Operational Stage (about 7 – 12 years) | Stage 3 of 4
Image: Mikail Akar, the 7-year-old being crowned the “Mini Picasso” (2020)
At the age of about 7 years old, the thinking processes of children change once again as they develop a new set of strategies which Piaget called “concrete operations”. These strategies are considered concrete because children can only apply them to immediately present objects. However, thinking becomes much more flexible during the concrete operational period because children lose their tendency to simply focus on one aspect of the problem, rather now, they are able to consider different aspects of a task at the same time. They now have processes like compensation and reversibility [as explained earlier in understanding volume], and they now succeed on conservation tasks. For example, when a round ball of clay is transformed into a sausage shape, children in the concrete operational stage will say, “It’s longer but it’s thinner” or “If you change it back, it will be the same.”
Conservation of number is achieved first [about 5 or 6 years], then this is followed by the conservation of weight [around 7 or 8], and the conservation of volume is fully understood at about 10 or 11 years old. Operations like addition and subtraction, multiplication and division become easier at this stage. Another major shift comes with the concrete operational child’s ability to classify and order, and to understand the principle of class inclusion. The ability to consider different aspects of a situation at the same time enables a child to perform successfully in perspective taking tasks [e.g. in the three mountains task of Piaget, a child can consider that she has one view of the model and that someone else may have a different view].
However, there are still some limitations on thinking, because children are reliant on the immediate environment and have difficulty with abstract ideas. Take the following question: “Edith is fairer than Susan. Edith is darker than Lily. Who is the darkest and who is the fairest?” Such a problem is quite difficult for concrete operational children who may not be able to answer it correctly. However, if children instead are given a set of dolls representing Susan, Edith and Lily, they are able to answer the question quickly. Hence, when the task is made a “concrete” one, in this case with physical representations, children can deal with the problem, but when it is presented verbally, as an abstract task, children have difficulty. Abstract reasoning is not found within the repertoire of the child’s skills until the latter has reached the stage of formal operations.
Revisions of the Concrete Operational Stage
A great amount of Piaget’s observations and conclusions about the concrete operational stage have been broadly confirmed by subsequent research. Tomlinson-Keasey (1978) found that conservation of number, weight and volume are acquired in the order stated by Piaget.
As in the previous stage, the performance of children in the concrete operational period may be influenced by the context of the task. In some context, children in concrete operational period may display more advanced reasoning that would typically be expected of children in that stage. Jahoda (1983) showed that 9-year-olds in Harare, Zimbabwe, had more advanced understanding of economic principles than British 9-year-olds. The Harare children, who were involved in the small business of their parents, had strong motivation to understand the principles of profit and loss. Jahoda set up a mock shop and played a shopping game with the children. The British 9-year-olds could not provide any explanation about the functioning of the shop, did not understand that a shopkeeper buys for less than he sells, and did not know that some of the profit has to be set aside for the purchase of new goods. The Harare children, by contrast, had mastered the concept of profit and could understand trading strategies. These principles had been grasped by the children as a direct outcome of their own active participation in running a business. Jahoda’s experiment, like Donaldson’s studies (1978), indicated the important function of context in the cognitive development of children.
IV. The Formal Operational Stage (12 years old) | Stage 4 of 4
During the third period of development, the Concrete operations stage, we have seen that the child is able to reason in terms of objects [e.g., classes of objects, relations between objects) when the objects are present. Piaget argued that only during the period of Formal Operations that young people are able to reason hypothetically, now they no longer depend on the “concrete” existence of objects in the real world, instead they now reason with verbally stated hypotheses to consider logical relations among several possibilities or to deduce conclusions from abstract statements [e.g. consider the syllogistic statement, “all blue birds have two hearts”; “I have a blue bird at home called Adornia”; “How many hearts does Adornia have?” The young person who has now reached formal operational thinking will give the correct answer by abstract logic, which is: “Two hearts!” Children within the previous stage will generally not get past complaining about the absurdity of the scenario.
Young people are now also better at solving problems by considering all possible solutions systematically. If requested to formulate as many combinations of grammatically correct words from the letters A, C, E, N, E, V, A, a young person at the formal operational stage could first consider all combination of letters AC, AE, AN, etc., verifying if such combinations are words, and then going on to consider all three letter combinations, and so on. In the earlier stages, children would attend to such tasks in a disorganised and unsystematic fashion.
Inhelder and Piaget (1958) explained the process of logical reasoning used by young people when presented with a number of natural science experiments. An example of one of their task, “The Pendulum Task” can be seen in Figure E.
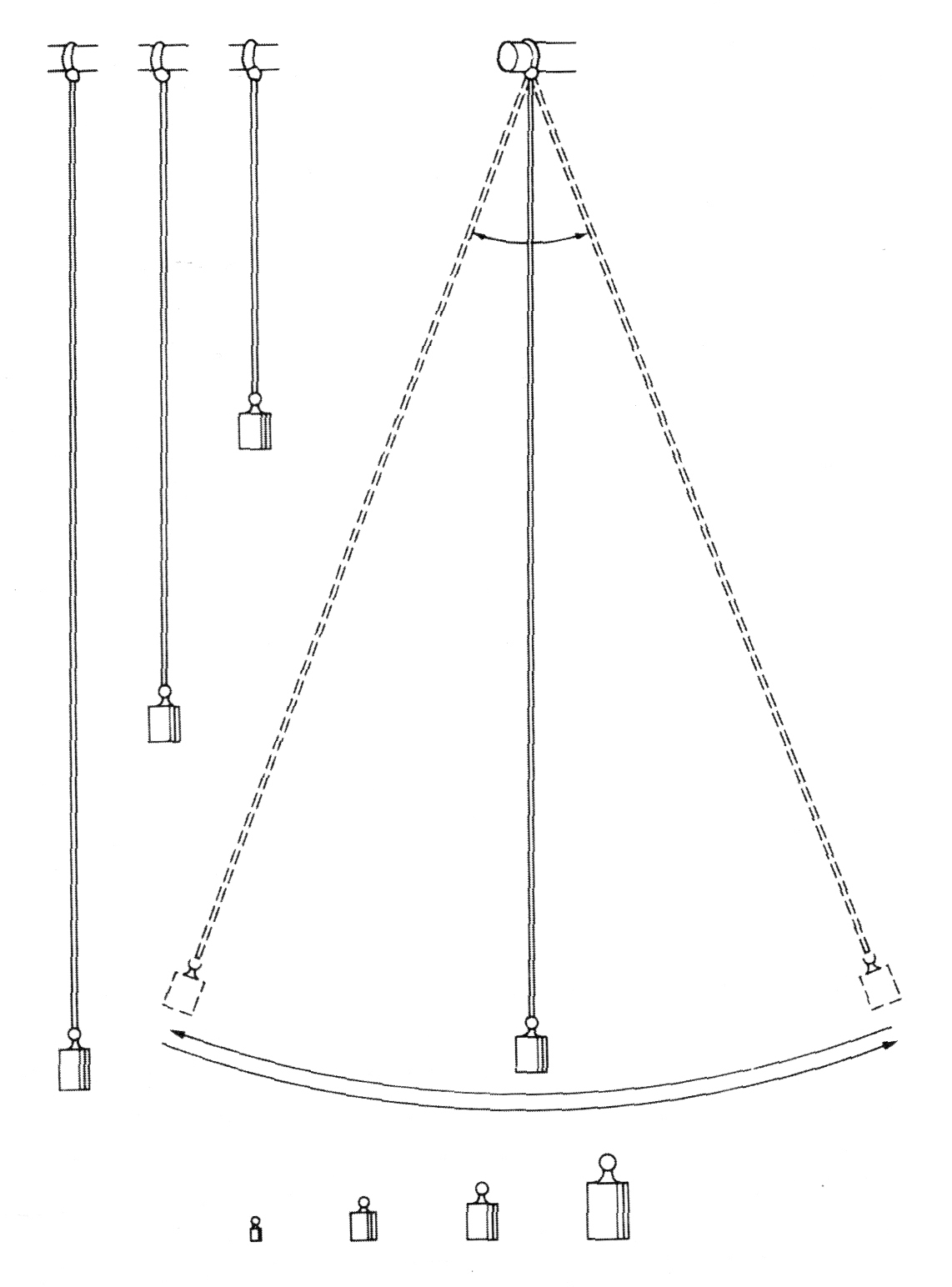
FIGURE E. The pendulum problem. The child is given a pendulum, different lengths of string, and different weights. She is asked to use these to work out what determines the speed of the swing of the pendulum (from Inhelder and Piaget, 1958).
The young person as the participant here is given a string [that can be shortened or lengthened], and a set of weights, and then asked to figure out what determines the speed of the swing of the pendulum. The possible factors are the length of the string, the weight at the end of the string, the height of the release point and the force of the push. In this particular scenario the solutions to the solving the problem are all in front of the participant, however the successful reasoning involves formal operations that would also have to incorporate a systematic consideration of various possibilities, the formulation of hypotheses (e.g., “What could happen if I tried a heavier weight?”) and logical deductions from the results of trials with different combinations of materials.
The other tasks investigated by Inhelder and Piaget (1958) included determining the flexibility of metal rods, balancing different weights around a fulcrum, and predicting chemical reactions. These tasks mimic the steps required for scientific inquiry, and Piaget argued that formal scientific reasoning is one of the most important characteristic of formal operational thinking. From his original work, carried out in schools in Geneva, Piaget claimed that formal operational thinking was a characteristic stage that children or young people reached between the ages of 11 and 15 years – having previously gone through the earlier stages of development.
Revision of the Formal Operational Stage
Piaget’s claim has been rectified by recent research, more researchers have found that the achievement of formal operational thinking is more gradual and haphazard than Piaget assumed – it may be dependent on the nature of the task and is often limited to certain domains.
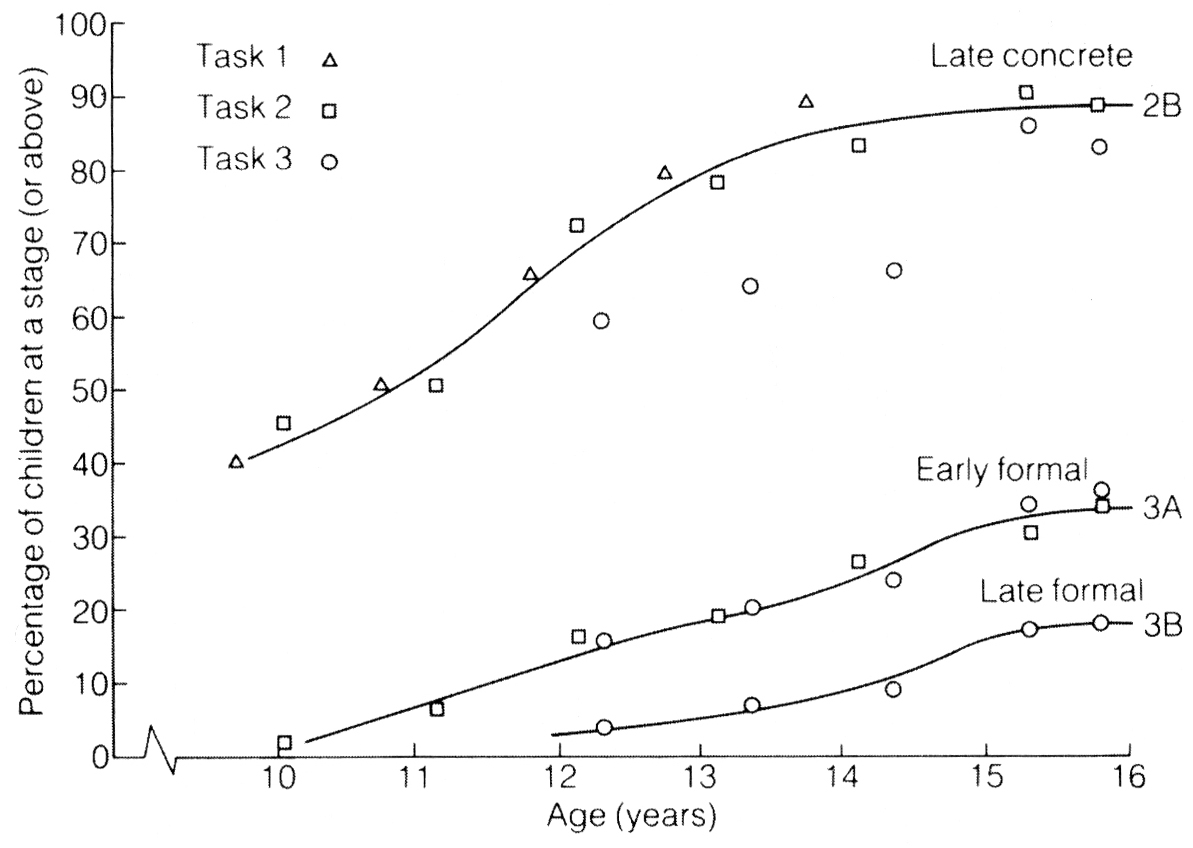
FIGURE F. Proportion of boys at different Piagetian stages as assessed by three tasks (from Shayer and Wylam, 1978).
Shayer et al. (1976; Shayer and Wylam 1978) gave problems such as the pendulum task [FIGURE E] to school children in the UK. Their results [see FIGURE F] showed that by 16 years of age only about 30% of young people had achieved “early formal operations” [Is this shocking compared to French speaking Europe where Piaget implemented his theory? Could this provide a partial explanation to the lack of personality, emotion, creativity, openness, depth and sophistication in some populations? Interesting questions…]. Martorano (1977) gave ten of Piaget’s formal operational tasks to girls and young woman aged 12 – 18 years in the USA. At 18 years of age success on the different tasks varied from 15% to 95%; but only 2 children out of 20 succeeded on all ten tasks. Young people’s success on one or two tasks might indicate some formal operational reasoning, but their failure on other tasks demonstrated that such reasoning might be limited to certain tasks or contexts. It is highly likely that young people only manage to achieve and apply formal reasoning across a range of problem tasks much later during their adolescence.
Formal thinking has been shown by some researchers as an ability that can be achieved through training, FIGURE G shows the results of such a study by Danner and Day (1977), where they mentored students aged 10 years, 13 years and 17 years in 3 formal operational tasks. As expected, training had a limited effect on the 10-year-olds, but it had marked effects at 17 years old. In summary, it seems that the period from 11 – 15 years signals the beginning of the potential for formal operational thought, rather than its achievement. Formal operational thought may only be used some of the time, in the domains we are generally familiar with, are trained in, or which have a great significance to us – in most cases formal thinking is not used. After all, we tend to know areas of life where we should have thought things out logically, but in retrospect realise we did not do so [without any regrets sometimes].
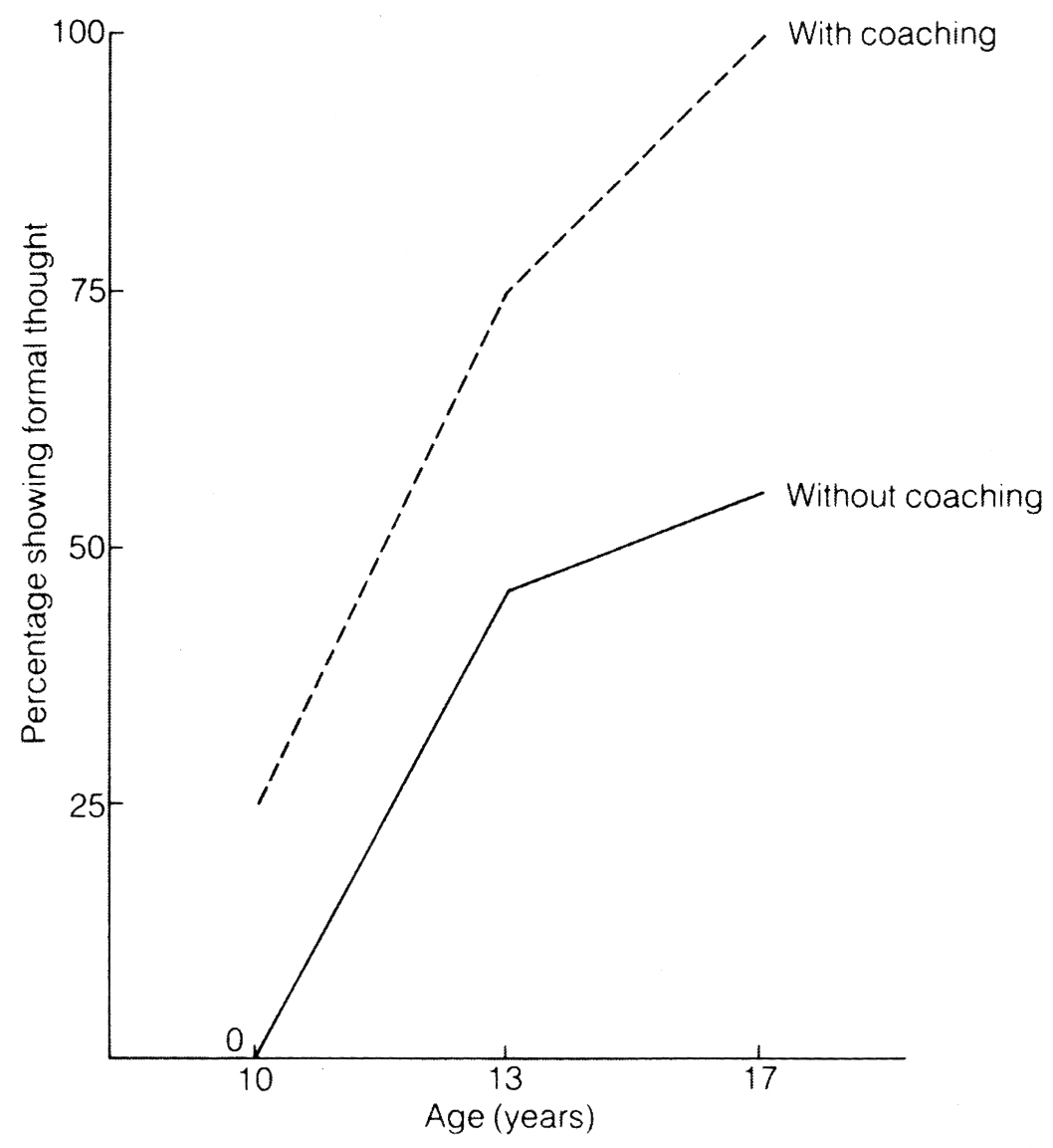
FIGURE G. Levels of availability of formal thought. Percentage of adolescents showing formal thought, with and without coaching (from Danner and Day, 1977).
The Educational Implications of Jean Piaget’s Theory of Cognitive Development
Piaget’s theory was planned and developed over many decades throughout his long life, and at first, it was slow to make any productive impact in the UK and the USA, but from the 1950s its ambitious, embracing framework for understanding cognitive growth was becoming the accepted and dominant paradigm in cognitive development.
Whatever the shortcomings are with Piaget’s theory, it impossible to deny his ingenious contributions, as his approach provided the most comprehensive description of cognitive growth ever put forward on earth. It has had considerable impact in the domains of education, most notably for child-centred learning methods in nursery and infant schools, for mathematics curricula in the primary school, and for science curricula at the secondary school level.
Piaget argued that young children’s thinking processes are quite different from that of an adult, and they also view he world from a qualitatively different perspective. It goes with the logic that a teacher must make a firm effort to adapt to the child and never assume that what may be appropriate for adults should necessarily be right for the child. The idea of “active learning” is what lies at the heart of this child-centre approach to education. From the Piagetian perspective, children learn better from actions rather than from passive observations [e.g., telling a child about the properties of a particular material is less effective than creating an environment in which the child is free to explore, touch, manipulate and experiment with different materials]. A good teacher should recognise that each child needs to construct knowledge for him or herself, and active learning results in deeper understanding.

“Our real problem is: what is the goal of education? Are we forming children who are only capable of learning what is already known? Or should we try to develop creative and innovative minds capable of discovery from the preschool age through life?” – Jean Piaget (1896 – 1980)
So, how can a teacher promote active learning on the part of the pupil? First, it should be the child rather than the teacher who initiates the activity. This should not lead us to allow the child a complete freedom to do anything they want to do, but rather a teacher should set tasks which are finely adjusted to the needs of their pupils and which, as a result, are intrinsically motivating to young learners. For example, nursery school classrooms can provide children with play materials that encourage their learning; set of toys that encourage the practice of sorting, grading and counting; play areas, like the Wendy House, where children can develop role-taking skills through imaginative and explorative play; and materials like water, sand, bricks and crayons that help children make their own constructions and create symbolic representations of the objects and people in their lives. From this range of experiences, the child develops knowledge and understanding for herself, and a good teacher’s role is to create the conditions in which learning may best take place, since the aim of education is to encourage the child to ask questions, try out experiments and speculate, rather than accept information and routine conventions unthinkingly – this also allows the child to learn and be creative about her subjective experience which is unique and different to any other child.
(1919) Jaroslava & Jiri, The Artist’s Children by Alphonse Mucha (1860 – 1939)
Secondly, a teacher should be concerned with the process rather that the end-product. This is in line with the belief that a teacher should be interested in the reasoning behind the answer that a child gives to a question rather than just in the correct answer. Conversely, mistakes should not be penalised, but treated as responses that can give a teacher insight into the child’s thinking processes at that time.
The whole idea of active learning resulted in changed attitudes towards education in all its domains. A teacher’s role is not to impart information, because in Piaget’s view, knowledge is not something to be transmitted from an expert master teacher to an inexpert pupil. It should be the child, according to Piaget, who sets the pace, where the teacher’s role is to create situations that challenge the child [creatively] to ask questions, to form hypotheses and to discover new concepts. A teacher is the guide in the child’s process of discovery, and the curriculum should be adapted to each child’s individual needs and intellectual level.
In mathematics and science lessons at primary school, children are helped to make the transition from pre-operational thinking to concrete operations through carefully arranged sequences of experiences which develop an understanding for example of class inclusion, conservation and perspective-taking. At a later period, a teacher can also encourage practical and experimental work before moving on to abstract deductive reasoning. Through this process, a teacher can provide the conditions that are appropriate for the transition from concrete operational thinking to the stage of formal operations.
The post-Piagetian research into formal operational thought also has strong implications for teaching, especially science teaching in secondary schools. The tasks that are used in teaching can be analysed for the logical abilities that are required to fulfil them, and the tasks can then be adjusted to the age and expected abilities of the children who will attempt them.
Considering the wide range of activities and interests that appear in any class of children, learning should be individualised, so that tasks are appropriate to individual children’s level of understanding. Piaget did not ignore the importance of social interaction in the process of learning, he recognised the social value of interaction and viewed it as an important factor in cognitive growth. Piaget pointed out that through interaction with peers, a child can move out of the egocentric viewpoint. This generally occurs through cooperation with others, arguments and discussions. By listening to the opinion of others, having one’s own view challenged and experiencing through others’ reactions the illogicality of certain concepts, a child can learn about perspectives other than her own [egocentric]. Communication of ideas to others also helps a child to sharpen concepts by finding the appropriate words.
“Everyone knows that Piaget was the most important figure the field has ever known… [he] transformed the field of developmental psychology.”
(Flavell, 1996, p.200)
“Once psychologists looked at development through Piaget’s eyes, they never saw children in quite the same way.”
(Miller, 1993, p.81)
“A towering figure internationally.”
(Bliss, 2010, p.446)
__________
(II) The Theory of Attachment in Emotional Development (John Bowlby)
If we pick up a new born baby , he/she will respond without any difference to us or to any other person. However, after 9 months, the same baby will have developed one or more selective attachments and will discriminate familiar faces to unfamiliar ones. So, if we were to pick up the baby again, we may face scenarios where he/she displays anxiety or cries, but if the mother or father picks her/him up, the baby will be reassured and pacified.
This section will explore and give an account of the development of attachment relationships between infants, parents, and other close primary caregivers. The significance of such attachments for development in adult life will also be considered, with its implication for the philosophy of education in sculpting the minds of tomorrow, along with some research on parenting styles analysing some of the factors affecting successful and less successful parenting.
The Development of Attachment Relationships: Attachment as an innate drive
The infant’s expression of emotions and the caregiver’s response to these emotions is the fundamental foundation of John Bowlby’s Theory of Attachment. Bowlby’s (1958, 1969 / 1982, 1973, 1980) theory was inspired and influenced by an exciting and creative range of disciplines including psychoanalysis, ethology and the biological sciences. Before Bowlby, the main assumption and view of the infant-mother attachment was that it was a “secondary drive” or a side-product of the infant associating the mother with the provision of physiological needs, such as hunger [Picture B – breast feeding image].

PICTURE B. Early theories of infant-mother attachment suggested that it was a secondary drive resulting from the mother satisfying the infant’s primary drives, such as hunger. / Photography: Jo Frances
Bowlby defied this logic, and argued convincingly that attachment was an innate primary drive in all infants, and while his theory went through many revisions over the years, this argument remained fundamental.
In Bowlby’s first version of his theory of attachment (Bowlby, 1958), the emphasis was on the role of behaviours resulting from our instincts [on how behaviours such as crying, clinging and smiling served the purpose of eliciting a reciprocal attachment response from the caregiver]:
There matures in the early months of life of the human infant a complex and nicely balanced equipment of instinctual responses, the function of which is to ensure that he obtains parental care sufficient for his survival. To this end the equipment includes responses which promote his close proximity to a parent and… evoke parental activity.
(Bowlby, 1958, p. 346)
However, in the 1969 version of his theory (1st volume of his trilogy, Attachment and Loss), Bowlby focussed on highlighting the dynamics of attachment behaviour, and switched to explaining the infant-mother tie in terms of a goal-corrected system which was triggered by environmental cues rather than innate instinctual behaviours. Whether attachment is instinctual or goal-corrected, we know that it eventually leads to the infant maintaining proximity to the primary caregiver.
Bowlby acknowledged that the development of an attachment relationship was not dependent purely upon the social and emotional interplay between infant and caregiver. Since we can only observe attachment behaviour primarily when the infant is separated from the caregiver, it is logically dependent upon the infant’s level of cognitive development in the ability for object permanence [i.e. the ability to represent an object (living or non-living) that is not physically present within the child’s proximity].
This seems to synchronise partly with Piaget’s outlook and theory of cognitive development, and indeed Bowlby was inspired by Jean Piaget, and based his argument on Piaget’s (1955) contention that this level of object permanence is not attained until the infant is approximately 8 months old. Furthermore, while children would be able to recognise familiar people before such age, they would still not miss the attachment figure and thus display attachment behaviour until they have reached the level of cognitive sophistication that comes with the ability to represent absent objects [and people, who are in the same class].
The Phases of Attachment: Development of Attachment Relationships
Let us imagine a classic example of a mother and child [about 1 – 2 year-old] in a park. What we might observe is that the mother is seated on a bench while the infant runs off to explore the area. Periodically, the child may be seen to stop and look back at the mother, and every once in a while may even return close to her, or make physical contact, staying close for a while before venturing off again. In most cases, the infant rarely goes beyond about 60 metres from the mother or primary caregiver, who may however have to go and retrieve the child if the distance gets too great or if the need to leave is imminent.
The scenario here from a developmental psychologist’s perspective is fairly simple; the infant is exploring the environment it is being exposed to inquisitively, and is using the mother as a “secure base” to which to return periodically for reassurance. This is one of the hallmarks of an “attachment relationship”. These observations of children in parks were made by a student of John Bowlby, Anderson (1972) in London, and the development of attachment has been described in detail by John Bowlby (1969).
Bowlby (1969, p. 79) described 4 phases in the development of attachment and subsequently extended it to a 5th.
The phases are:
I. The pre-attachment phase (0 – 2 months) is characterised by the infant showing hardly any differentiation in their responses to familiar or unfamiliar faces.
II. During the second phase (2 – 7 months), the foundations of attachment are being laid. Here infants start to recognise their caregivers, even if they still do not possess the ability to show attachment behaviours upon separation. The infant is also more likely to smile at the mother or important caregivers and to be comforted by them if distressed.

III. Clear cut attachment behaviours only start to appear after 7 months. At this phase, infants start to protest at being separated from their caregivers and become very wary of strangers [so called stranger anxiety] – this is often taken as a definition of attachment to caregiver and this onset of attachment happens from 7 – 9 months.
IV. When the attachment relationship has evolved into a goal-corrected partnership (from around 24 months / 2 years of age), [i.e. when the child also begins to accommodate to the mother’s needs, e.g. being prepared to wait alone if requested until the mother returns]. This is an important change because before this phase, the infant only saw the mother as a resource that had to be available when needed. Bowlby saw this as characterising the child at 3 years of age, although as mentioned from 2 years old babies can partly accommodate to verbal requests by mothers to await for her return (Weinraub and Lewis, 1977). From this phase onwards, the child relies on representation or internal working models of attachment relationships to guide their future social interactions.
V. The lessening of attachment is noticed as measured by the child maintaining proximity. The characteristics of a school-age child, and older, is the idea of a relationship based more on abstract considerations such as affection, trust, loyalty and approval, exemplified by an internal working model of the relationship.
Bowlby viewed attachment as a canalized developmental process where both the mainly instinctive repertoire of the new born and certain forms of learning are important in early social interactions. Certain aspects of cognitive sensori-motor development [as supported by Jean Piaget] are also fundamental for attachment. Until the developing infant can master the concept of cause-effect relations, and of the continued existence of objects [incl. persons] when out of sight, he or she cannot protest at separation and attempt to maintain proximity [note the importance of object permanence in emotional development and internal working models]. Hence, sensori-motor development is also a canalised process, and it should not be in opposition to an ethological and a cognitive-learning approach to attachment development.
Attachments: Between whom?
Many articles and textbooks have characterised the attachment relationship as mainly focussed on the mother (e.g. Sylvia and Lunt, 1981), and this may not be completely true, since many studies have suggested that early attachments are usually multiple, and although the strongest attachment is often to the mother, this need not always be so.
In a study conducted in Scotland, mothers were interviewed and asked to whom their toddlers showed separation protest (Schaffer and Emerson, 1964), the proportion of babies with more than 1 attachment figure increased from 29% when separation protest first appeared [about 7 – 9 months] to 87% at 18 months [1 and half year old]. It was also found that for about one third of babies, the strongest attachment seemed to be to someone other than the mother, such as father, or other trusted primary caregivers. In most cases, attachment were formed to responsive persons who interacted and played a lot with the infant; basic caregiving such as nappy changing was clearly not in itself such an important factor; and similar results were obtained by Cohen and Campos (1974).

Peinture: Sandrine Arbon
Studies in other cultures also support this conclusion, for example in the Israeli kibbutzim, young children spend the majority of their waking hours in small communal nurseries, in the charge of a nurse or metapelet. In a study of 1- and 2- year-olds reared in this way, it was found that the infants were very strongly attached to both the mother, and the metapelet; either could serve as a base for exploration, and provide reassurance when the infant felt insecure (Fox, 1977). In many agricultural societies, mothers tend to work in the fields, and often leave infants in the village, in the care of grandparents, or older siblings, returning periodically to breastfeed. In a survey of 186 non-industrial societies, it was found that the mother was rated as the “almost exclusive” caretaker in infancy in only 5 of them; hence other persons had important caregiving roles in 40% of societies during the infancy period, and in 80% of societies during early childhood (Weisner and Gallimore, 1977).
The Security of Attachment
Early infant-caregiver attachment relationships and the internal working models are the main aspects of Bowlby’s theory of attachment and have been given the greatest attention, with researchers developing 2 of the most widely used measuring instruments in developmental psychology to investigate Bowlby’s theoretical claims: the strange situation procedure to assess the goal-corrected system that evolved from the early attachment relationship, and the Adult Attachment Interview to assess internal working models.
Bowlby’s theory was focussed and interested with the making and breaking of attachment ties, probably because his experiences of working as a child psychologist exposed him to the negative consequences for emotional development of severe maternal deprivation [such as long term separation or being orphaned].
Nowadays, researchers and intellectuals are generally less concerned with whether a child has formed an attachment [since any child who experiences any degree of continuous care will become attached to the caregiver], but are rather more interested in the quality or security of the attachment relationship. This important shift in emphasis was due to the empirical work of Mary Ainsworth.
Ainsworth interest in the concept of attachment grew after working with Bowlby in London during the 1950s. Later, she moved to Uganda to live with the Ganda people where she made systematic observations of infant-mother interactions in order to investigate Bowlby’s goal-corrected attachment systems in action.
One factor that struck Mary Ainsworth (1963; 1967), was the lack of uniformity in infant’s attachment behaviour, in terms of its frequency, strength, and degree of organisation. Furthermore, these differences were not specific to Gandan infants, since she replicated these findings in a sample of children in the USA when she moved to Baltimore. These variations in attachment type had not been accounted for by John Bowlby’s Theory and hence, this led Ainsworth to investigate the question of individual differences in attachment.
Mary Ainsworth experience of working with Bowlby, along with her rich collection of data harvested over a period of many years, put her in a unique position in the development of attachment as an empirical field of research. Her contribution led to attachment issues becoming part of mainstream developmental psychology, rather than being simply confined to child psychiatry, and behind this achievement was an investigation of the development of attachment under normal family conditions and by developing a quick and effective way of assessing attachment patterns in the developmental laboratory.
Although the strange situation procedure (Ainsworth & Wittig, 1969) circumvented [found a way around] the need for researchers to conduct lengthy observations in the home, it was not developed simply for research convenience, but because there are problems in trying to evaluate attachment type in the child’s own home environment. For example, if a child becomes extremely distressed upon the mother moving to another room in their own home environment, this may be an indication of a less than optimal attachment achieved, because if a child feels secure then such a separation should not trigger any distress. The extensive experience of Ainsworth in observing infant-mother interactions enabled her to identify the situations that we most crucial in attachment terms, and therefore formed the basis of the strange situation procedure.
The Strange Situation Procedure
Ainsworth and her colleagues then developed a method for assessing the attachment strength of an individual infant towards her mother or caregiver (Ainsworth et al., 1978). The method is known as the Strange Situation, and has been widely used with 12 – 24 months old infants in many countries worldwide. To sum up, it is a method for checking in a standardised way, how well the infant uses the caregiver as a secure base for exploration, and is comforted by the caregiver after a lightly stressful experience.
The strange situation assesses infants’ responses to separations from and subsequent reunions with, the caregiver [mother here], and their reactions to an unfamiliar woman [the so-called “stranger”]. In the testing room, there are only 2 chairs [one for the mother and one for the stranger] and a range of toys with which the infant can play.
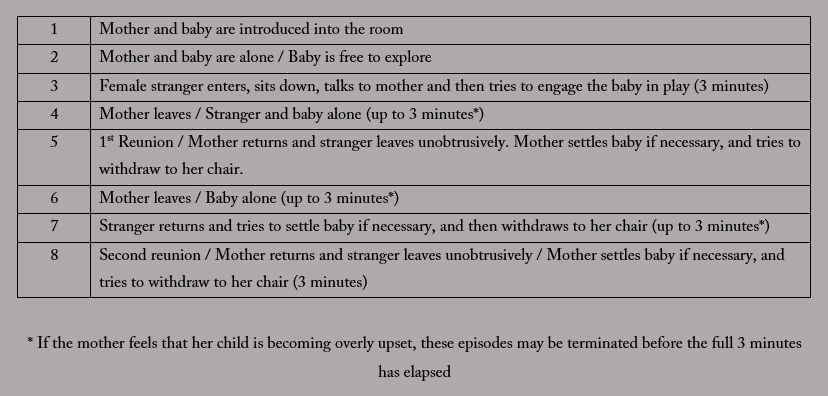
Table A. The Strange Situation Procedure
As Table A shows, the episodes are ordered so that the infant’s attention should shift from the exploration of the environment to attachment behaviour towards the caregiver as the Strange Situation proceeds. The most crucial points are the infant’s responses to the 2 reunion episodes, and form the basis for assessing an infant’s security of attachment. The coding scheme for security attachment was developed by Ainsworth et al. (1978) and describes infant behaviour according to 4 indices:
1) Proximity-seeking
2) Contact-maintenance
3) Resistance
4) Avoidance
Referring to Table A, in a well-functioning attachment relationship, it would generally assumed that the infant would use the mother as a base to explore [Episodes 2, 3 and the end of Episode 5], but be stressed by the mother’s absence (Episodes 4, 6 and 7; these episodes are cancelled if the infant is overly distressed or the mother wants to return sooner]. Special attention is also given to the infant’s behaviour in the reunion episodes (5 and 8), to see if her or she is effectively comforted by the mother. Based on those measures, Ainsworth and others distinguished a number of different attachment types.
The 4 primary ones are:
Type A – Insecure Avoidant Attachment
Insecure-Avoidant (Type A) infants display high levels of environment-directed behaviour to the detriment of attachment behaviour towards the caregiver [i.e. Avoidant (A) – avoids caregiver and explores environment]. The Insecure Avoidant Types display little if any proximity-seeking behaviour, and even tend to avoid the caregiver, by averting gaze or turning or moving away, if the caregiver attempts to make contact. Throughout the whole process of the Strange Situation, Insecure Avoidant infants appear completely indifferent toward the caregiver, and treat both the latter and the stranger is very similar ways; hence, these infants may show less avoidance of the stranger than of the caregiver.
Note that conversely, the (Type C) Insecure Resistant / Ambivalent Attached infants show high levels of environmental-directed behaviour to the detriment of the caregiver [the complete opposite to Type A].
Type B – Secure Attachment
When the dynamics of the attachment relationship is a balance between environmental exploration and attachment behaviour directed towards the caregiver [See PICTURE C], then the securely attached infants are considered as having the right balance.
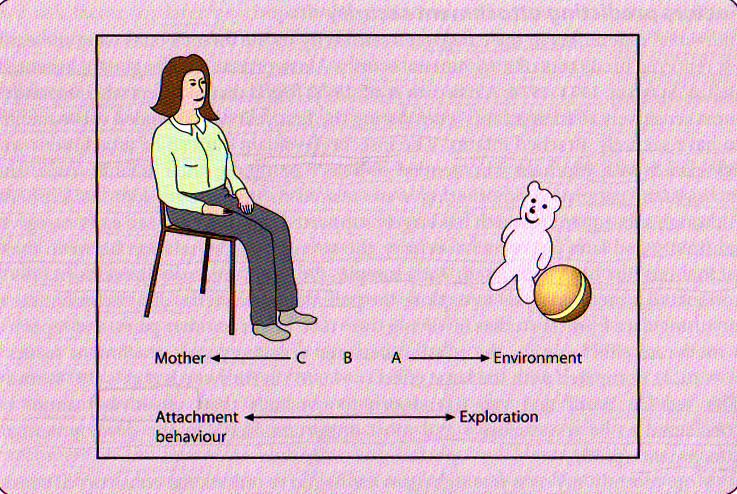
PICTURE C. Attachment as a balance of behaviour directed toward mother and the environment. Source: Adapted from Meins (1997).
The presence of the caregiver in the pre-separation episodes affords them the security to turn their attention to exploration and play, with the confident knowledge that the caregiver will be available for comfort or support should it be required. However, attachment behaviour is triggered in securely-attached infants during the separation episodes, leading to seek contact, comfort, proximity or interaction with the caregiver when they return. Securely attached infants may or may not become distressed upon separation from caregivers, and this makes the infants’ response to separation a relatively unreliable and poor indicator of attachment security. However, regardless of their response to separation, securely attached children are marked by their positive and quick response to the caregiver’s return, displayed generally by their readiness to approach, greet and interact with the caregiver.
It important to note that Type B [Secure] Attachment is the only “secure” attachment in the group, all the rest are insecure attachment types, and in contrast to Type B, they have their balance of infant attachment tipped to either extreme [i.e. Avoidant (A) – avoids caregiver and explores environment / Resistant (C) – avoids environment and exhausts caregiver]
Type C- Insecure Resistance / Ambivalent
Insecure-resistant infants are over-involved with [to the point of exhausting] the caregiver, showing attachment behaviour even during the pre-separation episodes, with little or no interest in exploring the environment. The Insecure Resistant (Type C) infants tend to become extremely distressed upon separation, however, the over-activation of their attachment system hampers their ability to be comforted by the caregiver upon reunion – this leads to angry or petulant behaviour, with the infant resisting contact with and from the caregiver [in extreme cases this manifests itself as tantrum behaviour where the caregiver may sometimes be hit or kicked by the infant].
Type D – Insecure Disorganised
Besides the original 3 categories mentioned above distinguished by Ainsworth et al. (1978), Main and Solomon (1986, 1990) established a fourth category, Type D [Insecure Disorganised Attachment] for infants whose behaviours appeared not to match any of the A [Avoidant], B [Secure] and C [Resistant/Ambivalent] categories. These insecure-disorganised infants look disoriented during the strange situation procedure, and display no clear strategy for coping with separations from and reunion with their caregivers. Infants classified as insecure-disorganised may simultaneously display contradictory behaviour during the reunion episodes, such as seeking proximity while also displaying obvious avoidance [e.g. backing to which the caregiver or approaching with head sharply averted]. Insecure-disorganised infants (Type D) may also react to reunion with fearful, stereotypical or odd behaviours [e.g. rocking themselves, ear pulling, or freezing]. Main and Hesse (1990) argued that, although the classification criteria for insecure-disorganised attachment are diverse, the characteristic disorganised behaviours all include a lack of coherence in the infant’s response to attachment distress and betray the “contradiction or inhibition of action as it is being undertaken” (p.173).
Main and her colleagues (1985) believe the Type D [Insecure-disorganised ] is a useful extension of the original Ainsworth classification.
There are many subtypes of these main types, however most studies do not refer to them, and in older studies, type D babies [who are often difficult to classify as they do not show a clear pattern] were ‘forced’ into 3-way and 4-way classifications.
In most cases, type B babies (secure – considered as most desired, i.e. “normal” / although debated] are compared with types A and C [inscure-avoidant and insecure-resistant/ambivalent], and the type B [secure-attachment] tends to be seen as developmentally normal, or advantageous. Many criticisms have been made of the attachment typing resulting from the Strange Situation procedure (Lamb et al., 1984), particularly of the earlier work that was based on small samples, and of the normative assumption that “B is best”. They also pointed out the procedure only measures the relationship between mother and infant, and not the characteristics of the infant. Since attachment security is the dyadic measure, infant-mother attachment type is not necessarily the same as infant-father attachment type. In fact, many studies have found that the attachment type to father is not related to that with the mother; meta-analyses (Fox et al., 1991; van Ijzendoorn and De Wolff, 1997) found a very modest association between the two.
However, the strange situation procedure is today a commonly and internationally used technique. One of the most important test of utility of attachment types is that it should allow us to predict other aspects of development, and we now have considerable evidence for this (see Bretherton and Waters, 1985 and Waters et al., 1995, for reviews).
Kochanska (2001) followed infants longitudinally from 9 to 33 months and observe their emotions in standard laboratory episodes designed to elicit fear, anger or joy. Over time, type A (Avoidant – towards caregiver) infants became more fearful, type C (Resistant/Ambivalent – exhausts caregiver) infants became less joyful, type D (Disorganised – does not fit in A, B or C behavioural categories) infants became more angry; whereas type B (Secure) infants showed less fear, anger or distress. Using the strange situation procedure, secure attachment to mother at 12 months has been found to predict curiosity and problem solving at age 2, social confidence at nursery school at age 3, and empathy and independence at age 5 (Oppenheim et al., 1988), and a lack of behaviour problems (in boys) at age 6 (Lewis et al., 1984).
Is the Strange Situation valid across populations worldwide?
Van Ijzendoorn and Kroonenberg (1988) provided a cross-cultural comparison of strange situation studies in a variety of different countries. In American studies, some 70% of infants were classified as securely attached to their mothers (type B), some 20% as Type A, and some 10% as Type C. However, German investigators found that some 40-50% of infants were of Type A (Grossman et al., 1981), while a Japanese study found 35% to be of Type C (Miyake et al., 1985). These percentages do raise the question about the nature of “insecure attachment”: is it a less satisfactory mode of development or are these just different styles of interaction?
Takahashi (1990) argued that the Strange Situation must be interpreted carefully when it is applied across cultures. He found that Japanese were excessively distressed by infant alone episode (episode 6 – Table A), because generally in Japanese culture babies are never left alone at 12 months. This is the reason why fewer Japanese babies scored B (Secure). It is also important to note, that there was no chance for them to show avoidance (and score A – insecure avoidant), since the mother seeing the level of distress went straight on without hesitation to pick up the baby. This may also be possible explanation as to why many Japanese babies were C (Insecure Resistant/Ambivalent) at 12 months [still they are not at 24 months, nor are adverse consequences apparent]. This distortion can be avoided by virtually omitting episode 6 (see Table A) for such babies. Rothbaum et al. (2000) do take a more radical stance, in comparing the assessment security in the USA and Japan. They argue that these two cultures put different cultural values on constructs such as independence, autonomy, social competence and sensitivity; such that some fundamental tenets of attachment theory are called into question as cross-cultural universals.
Cole (1998) suggested that we need information of the geographical trends in socio-behavioural patterns [culture, heritage, language, arts, etc] under study if we are to understand the nature of the everyday interactions that shape the development of young children in relation to their caregivers. The strange situation may be a valid indicator but we at least need to redefine the meaning of the categories “avoidant, secure and resistant / ambivalent” according to the geographical socio-behavioural patterns [culture]. He also argued that although it is a standardised test, strange situation is really a different situation in different environmental circumstances. However for successful use of the strange situation in a non-western culture [one that is not of Western European heritage], we can take a look at the Dogon people of Mali.
Infant-mother attachment among the Dogon of Mali
The study we are about to discuss is a very rare one among its kind which took place among the Dogon people of Eastern Mali, a primarily agrarian people living by subsistence farming of millet and other crops, as well as cash economy in towns [see PICTURE D].
PICTURE D. Dogon mother spinning cotton with child on her lap
The study was carried out in 2 villages with a total population of about 400, and one town population of 9000, with the researchers attempting to get a complete coverage of infants born between mid-July and mid-September 1989. Not all infants could take part, due to relocation or refusal, and the researchers excluded 2 infants who had birth defects, and 8 suffering from severe malnutrition. In addition, after recruitment two infants die before or during the two-month testing period. Finally, 42 mother-infant pairs took part and provide a good quality data. The infants were 10 to 12 months old at the time of testing.
The Dogon are a polyamorous society, and mothers typically live in a compound with an open courtyard, often shared with co-wives. There was some degree of shared care of infants, about one half were cared for primarily or exclusively by the mother, about one third primarily by the maternal grandmother with a mother however being responsible for breastfeeding (see PICTURE E).
PICTURE E. Dogon mother breastfeeding her child.
Breastfeeding is a normative response by the mother to signs of distress in in the Dogon infants. Three related features of infant care in the Dogon – frequent breastfeeding on demand, quick response to infant distress, and constant proximity to the mother or caregiver – are seen as adaptive and there is high infant mortality [as in some other traditional African cultures].
The researchers have several objectives in mind, they wish to see if the strange situation could be used successfully in Dogon culture; one distribution of attachment types was obtained; whether infant security correlated with maternal sensitivity – a test of the Maternal Sensitivity Hypothesis; whether infant attachment type related to patterns of attachment-related communications in mother-infant interaction – the test of what the authors call the Communication Hypothesis; and to see if frightened or frightening behaviour by the mother predicted disorganised infant attachment.
Three situations were used to obtain relevant data, the behaviour being recorded on videotape in each case. One was rather new – the Weigh-In, part of the regular well-infant examination, in which the mother handed over the infant to be weighed on a scale – and mildly stressful separation for the in, especially in Dogon culture. The other two were more standard – the strange situation, carried out in an area of courtyard separated off by hanging mats; and two 15 minute observations in the infant’s home, and the mother was cooking, bathing/caring for the infant.
The following data were obtained:
- Infant attachment classification (from the strange situation)
- A rating of infant security on a 9-point scale (from the strange situation)
- Mother and infant communication related to attachment, coded by 5-point Communications Violations Rating scales (from the Weigh-in)
- Maternal sensitivity, rated in terms of promptness, appropriateness and completeness of response to infant signals (from the home observations)
- Frightened or frightening behaviours by the mother, such as aggressive approach, disorientation, trance state, rough handling as if baby is an object, on a 5-point scale (from the home observations and the Weigh-In).
[REMEMBER!!!! [although we are quite sure you know this already] : “r” is known as the correlation coefficient and tells us 2 things: (i) Direction of Relationship + or – & (ii) Strength of Relationship : +or- .1 is a small effect / +or- .3 is a medium effect / +or- .5 is a large effect | and p-value is the critical decider of whether to reject Null Hypothesis( i.e. the scenario we rightly thought would be opposite to our predictions) if p small enough (if p < .05 we say results were statistically significant, if p < .01 we say it is HIGHLY statistically significant) we reject the Null Hypothesis [both cases].
The strange situation was found to be feasible, following quite standard procedures. The distribution of attachment types was 67% B (Secure), 0% A (Avoidant), 8% C (Resistant/Ambivalent), and 25% D (or on a forced 3-way classification, 87% B, 0% A and 13% C). This is quite unusual in having no avoidant (A) classifications; D is high but not significantly greater than Western norms.
The Maternal Sensitivity Hypothesis only received weak support. The correlation between infant security and maternal sensitivity was r = 0.28, and with p < .10; the difference in means between attachment classifications was not statistically significant (B=5.26, C=5.00, D=4.20).
The Communications Hypothesis did get support. Infant security correlated -.54 with Communications Violations (p < .001), and the attachment classifications differed significantly (B=2.66, C = 3.50, D = 3.89; p < .01).
Finally, frightened or frightening behaviour by the mother correlated r = -.40 (p < .01) with infant security, and was particularly high in children with disorganised attachment (B= 1.23, C = 1.33, D = 2.35; p < .01).
Besides demonstrating the general application of the strange situation procedure in a nonwestern group with socio-behavioural patterns very different to our own, the findings provides support for the Communication Hypothesis. The case here would have been stronger if the different kinds of communication patterns for each attachment classification had been described in more detail. For example, that insecure resistant / ambivalent (C) attachment type infants would be inconsistent and often unable to convey their intent, or to terminate their own or another’s arousal, whereas insecure disorganised (D) attachment type infants would “manifest contextually irrational behaviours and dysfluent communication” (p. 1451). As it is, the main findings show that insecure infants show more communications violations, do not describe the detailed typology. Indeed, since some of the Communications Violations rating scales were of “avoidance, resistance and disorganisation” (p. 1456), there is a possible danger of conceptual overlap between this scale and the attachment classifications.
Although support for the Maternal Sensitivity Hypothesis was we, the correlation of r = .28 is in line with the average of r = .24 found in the meta-analysis by De Wolff and Van Ijzendoorn (1997) on mainly Western samples. The researchers used a multiple regression analysis to examine the contributions of both maternal sensitivity and mothers frightened/frightening behaviour, to attachment security. They found that the contribution of maternal sensitivity remain modest, whereas the contribution of mothers frightened/frightening behaviour was substantial and significant; ratings of maternal sensitivity do not normally take account of mothers frightened/frightening behaviour, and the researchers suggest that this might explain the modest effects found for maternal sensitivity to date.
The absence of avoidant (A – avoids caregiver and favours exploration) type infants is interesting and the researchers argue that, given the close contact mothers maintained with the Dogon infants, and the normal use of breastfeeding as a comforting activity, it would be very difficult for it Dogon infant to develop an avoidant strategy [this may have some similarity with the low proportion of A-type in Japanese infants). If avoidant (A) attachment is a rare or absent when infants nursed on demand (which probably characterises much of human evolution), this might suggest that A type attachment was and is a rare except in Western samples in which infants tend to be fed on schedule, and often by bottle rather than breast, so that the attachment and feeding systems are effectively separated.
Most Dogon infants showed secure (B) attachment, but 25% scored as disorganised (D) [though mostly with secure as the forced 3-way classification]. The researchers comment that the frightened or frightening behaviours were mild to moderate, and did not constitute physical abuse. But why should mothers show these sorts of behaviour at all? An intriguing possibility is that it is related to the high level of infant mortality prevalent in the Dogon. About one third of infants died before five years of age, and most mothers will have experience in early bereavement. Unresolved loss experienced by a mother is hypothesised to disorganised (D) attachment; perhaps, frightened behaviours are more rational or expected, when the risk for infants are so much higher.
This study to great efforts to be sensitive to the geographically specific socio-behavioural patterns (culture) of the venue, when using procedures and instruments derive mainly from Western samples. A Malian researcher assisted in developing the maternal sensitivity coding, and Dogon women acted as strangers in the strange situation procedure. The Weigh-In and home observations were natural settings. The authors comment, however, that future work might make more effort to tap the perceptions of mothering and attachment held by the Dogon people themselves, in addition to the constructs coming from Western psychology.
(True, M. M., et al, 2001)
Back Home in the West: Why do infants develop certain attachment types?
Individual differences in the caregiver’s sensitivity to infant’s cues were the earliest reported predictors of attachment security. Ainsworth and colleagues (Ainsworth, Bell & Stayton, 1971, 1974; Ainsworth et al., 1978) found that mothers who responded most sensitively to their infants’ cues during the first year of life tended subsequently to have securely attached infants. The insecure-avoidant (Type A) pattern of attachment was associated with mothers who tended to reject or ignore their infants’ cues, and inconsistent patterns of mothering were related insecure-resistant/ambivalent (Type C) pattern of attachment. Although further research has largely supported this link between early caregiver sensitivity and later attachment security, the strength of the relation between these factors has not been replicated. For example, De Wolff and van Ijzendoorn (1997) conducted a meta-analysis to explore the parental antecedents of attachment security using data from 21 studies involving over 1000 infant-mother says, and reported a moderate effect size for the relation between sensitivity and attachment security (r = 0.24), compared with the large effect (r = 0.85) in Ainsworth et al.’s (1978) study. This led De Wolff and van Ijzendoorn to come to the conclusion that “sensitivity cannot be considered to be the exclusive and most important factor in the development of attachment” (p. 585).
It seemed that the construct of sensitivity might have been responsible for the result, so we return to Ainsworth et al.’s (1971, 1974) original definitions in order to have a better understanding of predictors of attachment security. In this research, we were particularly influenced by Ainsworth’s focus on the caregiver’s ability not merely to respond to the infant, but to respond in a way that was consistent with the infants cue. For example, Ainsworth et al., (1971) describe how mothers of securely attached infants appeared “capable of perceiving things from the child’s point of view” (p. 43), whereas maternal insensitivity involve the mother attempting to “socialise with the baby when he is hungry, play with him when he is tired, and feed him when he is trying to initiate social interaction” (Ainsworth et al., 1974, p. 129). Meins et al. (2001) verse argued that the critical aspect of sensitivity was the caregiver’s ability to “read” the infant’s signals accurately so that the response could be matched to this passive cue from the child.

In order to test this proposal, Meins et al. (2001) obtain measures of mothers’ ability to read their 6-month-olds’ signals appropriately (so called mind-mindedness), and investigated the comparative strength of mind-mindedness versus general maternal sensitivity in predicting subsequent infant-mother attachment security. Meins et al. reported that maternal mind-mindedness was a better predictor of attachment security 6 months later than was maternal sensitivity, with mind-mindedness accounting for almost twice the variance in attachment security than that accounted for by sensitivity.
This seems like a strong conclusion, since the genetic factors have been accounted for and do not contribute to attachment type as van Ijzendoorn et al. (2000) argued that it has a modest if any influence on attachment type. This can be confirmed from a twin study conducted by O’Connor and Croft (2001) when they assessed 110 twin pairs in the strange situation and found concordance of 70% in monozygotic twins and 64% in dizygotic twins – not significantly different. The model suggested estimates of only 14% of variance in attachment type due to genetics, 32% to shared environment, and 53% in non-shared environment.
A study of attachments formed by babies to foster mothers (Dozier et al., 2001) found as good a concordance between mothers’ attachment state of mind (from the Adult Attachment Interview, see below) and infant attachment type from the strange situation, as for biological mother-infant pairs, once again suggesting little genetic influence on attachment type.
So, it is fairly accepted today that mothers’ mind-mindedness is an important construct and it is defined as the mother treating her infant as an individual with a mind, instead of just an organism or small creature with needs to be satisfied. The emphasis should be on responding to the infant’s inferred state of mind, rather than simply their behaviour. In a longitudinal study of 71 mother-infant pairs, they found that maternal sensitivity (responding to infant cues) and some aspects of mind-mindedness, especially appropriate mind-related comments by the mother, measured at six months, both independently predicted security of attachment at 12 months. True et al., (2001) also found evidence that mothers’ frightened or frightening behaviour may also contribute independently to attachment security (Refer to Dogon Study above – Picture D and Picture E).
We should also take note that a huge amount of variance in attachment type appears to be related non-shared environment, and this cannot be explained by generalised maternal sensitivity. It is highly probable that, mothers are more sensitive and behave differently to some infants than others, depending on birth order, gender and infant characteristics, suggesting the need for family systems on these issues (van Ijzendoorn et al., 2000).
Attachment Beyond Infancy & The Internal Working Model
The attachment theory proposes that children use their early experiences with their caregivers to form internal working models (Bowlby, 1969 /1982, 1980) which incorporate representations of themselves, their caregivers, and their relationships with others. These internal working models will then be used by the child as templates for interacting with others. Consequently, because of the sensitive, loving support that securely attached children’s caregivers have supplied, these children are self-confident and have a model of themselves as being worthy; they therefore expect others to behave in a sensitive and supportive fashion. Conversely, given the patterns of interaction typically experienced by avoidant and resistant infants, insecurely attached children expect people to be rejecting, or inconsistent and ambivalent when interacting with them.
The strange situation measures security of attachment in terms of behaviours; especially how the infant behaves at a reunion of the separation. The strange situation procedure is generally used with infants between the ages of 12-24 months old. For 3 – 6 year-olds, variants of the strange situation, such as a reunion episodes after separation, have been used with some success (Main and Cassidy, 1988).
Research during the last 10 years has seen attachment become a life-span construct with corresponding attempts to measure it at different developmental stages (see Melhuish, 1993, for a review). It has been revealed that as infants grow older, in Bowlby’s 4th and 5th stages, attachment relationships become less dependent on physical proximity and overt behaviour, and more dependent on abstract qualities of the relationship such as affection, trust, approval, internalised in the child and also in the adult.
Research has revealed that it is useful to think of internal representations of the relationship in the child’s mind; the child is thought of as having an internal working model of his or her relationship with the mother, and with other attachment figures (Bowlby, 1988; Main et al., 1985). These are characterised as cognitive structures embodying the memories of day-to-day interactions with the attachment figure. They may be ‘schemas’ or ‘event scripts’ that guide the child’s action with the attachment figure, based on their previous interactions and the expectations and affective experiences associated with them.
Different attachment type would be expected to have differing working models of the relationship. Secure (Type B) attachment would be based on models of trust and affection [and a Type B infant would be able to communicate openly and directly about attachment-related circumstances, such as how they felt if left alone for a while]. By contrast, a boy or girl with an Insecure Avoidant (Type A) attachment may have an internal model of his/her mother that leaves the child without any expectancy of secure comforting from the latter when he/she is distressed [the mother may in fact reject his/her approaches]. The child’s action rules then become focused on avoiding her, thus inhibiting approaches to her that could be ineffective and instead lead to further distress; and this can be problematic, as there is less open communication between mother and son, and their respective internal working models of each other are not being accurately updated.
Insecure Resistant / Ambivalent (Type C) infants might not know what to expect from their mother, and they in turn would be inconsistent in their communication with the latter and often unable to convey their intent.
PICTURE F. Boy by Land Rover: A picture from the Separation Anxiety Test
Over the last 15 years, researchers have attempted to measure attachment quality in older children [as much as the empirical methods allowed them to do in terms of construct validity and internal consistency], by trying to tap in to their internal working models (Stevenson-Hinde and Verschueren, 2002). One of the methods used involved narrative tasks, often using doll-play; children use a doll family and some props and complete a set of standardised attachment related story beginnings. Another method used has been the Separation Anxiety Test, in which children or adolescents respond to photographs showing separation experiences [see Picture G for an example]. The child is questioned about how the child in the photograph would “feel and act”, and then how he/she [the participating child] would feel and act if in that situation (Main et al., 1985). This test was found to have a good rater reliability and consistency for 8 to 12-year-olds. Large differences in responses between children having clinical treatment for behaviour disturbance and a normal control group was found (See Table B)
TABLE B. Two protocols from the Separation Anxiety Test
Securely attached children generally acknowledge the anxiety due to the separation but come up with feasible coping responses; insecurely attached children generally deny the anxiety, or give inappropriate or bizarre coping responses.
The Adult Attachment Interview
The internal working models of relationships can normally be updated or modified as new interactions develop. It is likely possibility that for younger children, these changes must be based on actual physical encounters. However, the Main et al. (1985) suggested that in adolescents or adults who have achieved formal operational thinking [Jean Piaget’s 4th and final stage at around the age of 12 as explained in our essay], it is possible to change / modify their internal working models without the need for such direct interaction. In order to measure attachment in older adolescents and adults, they developed the Adult Attachment Interview. This is a semi-structured interview that proves memories of one’s own early childhood experiences. The transcripts are coded, not on the basis of experiences themselves, so much as on how the person reflects on and evaluate them, and how coherent total account is [Adults’ attachment classifications are not based on the nature of their actual childhood experiences, but on the way they represent these experiences, be they good or bad]. They are also generally asked to describe their childhood relationships with mother and father, and to recall times when they were separated from their parents or felt upset or rejected. There are specific questions that also deal with experiences of loss and abuse. According to their responses during the AAI, Allsopp placed into one of the 4 attachment categories: (i) Autononous, (ii) Dismissing, (iii) Preoccupied [Or Enmeshed] and (iv) Unresolved
(i) Autonomous Attachment
Autonomous adults are able to give coherent, well-balanced accounts of their attachment experiences, showing clear valuing of close personal and meaningful relationships [note meaningful subjectively to the individual]. These adults classified as autonomous may have experience problems in childhood, or even had a very difficult or abusive upbringings, but they can generally have an open conversation and talk openly about the negative experiences and most seem to have managed to resolve any early difficulties and conflicts. In contrast to the open and balanced way in which autonomous adults talk about childhood experiences, adults in the remaining three categories have incredible difficulties in talking about attachment relationships.
(ii) Dismissing Attachment
Dismissing adults deny the importance of attachment experiences and insist they cannot recall childhood events and emotions, or provide idealised representations of the attachment relationship that they are unable to corroborate the real-life events. [i.e. dismiss attachment relationship as of little importance, concern or influence
(iii) Preoccupied [or Enmeshed] Attachment
Preoccupied adults lack the ability to move on from the childhood experiences, and are still overinvolved with issues relating to the early attachment relationship [generally preoccupied with dependency on their own parents and still struggle to please them].
(iv) Unresolved Attachment
The final category is reserved for adults who are unable to resolve feelings relating to the death of a loved one or to abuse they may have suffered [people who have not come to terms with a traumatic experience, or work through the mourning process]
It is to be noted that, people from lower socio-economic groups are slightly more likely to score as Dismissing. However the large difference is in people receiving clinical treat, the great majority of whom do not score as Autonomous on the AAI.
Are attachments stable over time? From Infancy to Adult Attachment Type
The main question should be asking ourselves is does the security of attachment change the life, or does infant-parent attachment set the pattern not only for later attachment in childhood, but even for one’s own future parenting? As attachment has become lifespan construct, these questions have generated considerable research and debate.
Many studies have now spanned a period of some 20 years to examine whether strange situation classification in infancy predicts Adult Attachment Interview (AAI) classification as young adults (Lewis et al., 2000; Waters et al., 2000). The outcome is varied, but some of these studies have found significant continuity of the 3 main attachment types; that is, from Secure to Autonomous; Avoidant to Dismissive, and Resistant (Ambivalent) to Enmeshed. Several studies have also found relationships between discontinuities in attachment classification, and negative life events such as the experience of parent divorce.
Relationship between Adult Attachment Interview (AAI) and Infant-Parent Attachments
Adult Attachment Interview (AAI) and classifications have been found to relate systematically to the security of the infant-parent attachment relationship. Autonomous parents are more likely to have securely attached infants, and parents in the 3 non-autonomous group. Dismissing, Preoccupied and Unresolved are much more likely to form insecure attachment relationships with their infants. This relationship has been identified for both patterns of infant-mother (e.g. Fonagy et al., 1991; Levine et al., 1991) and infant-father (Steele et al., 1996) attachment. Furthermore, unresolved maternal AAI classification has been identified as a predictor of insecure-disorganised attachment (Main & Hesse, 1990; van Ijzendoorn, 1995). Thus, the way in which a parent represents their own childhood attachment experiences is related to the types of relationship formed with their children.
Are attachment stable over generations?
On top of the degree of continuity over time for an individual’s attachment typing, there is also evidence for the transmission of attachment type across generations; specially from the parent’s AAI (Adult Attachment Interview) Coding and their infant’s strange situation coding. Main et al. (1985) had reported some evidence for such a link, and indeed the AAI coding system is based on it; it was argued that Autonomous adults would end up with Secure infants; Dismissing adults with Avoidant infants, Enmeshed adults with Resistant (Ambivalent) infants; and Unresolved adults would have Disorganised infants. [See Table C].
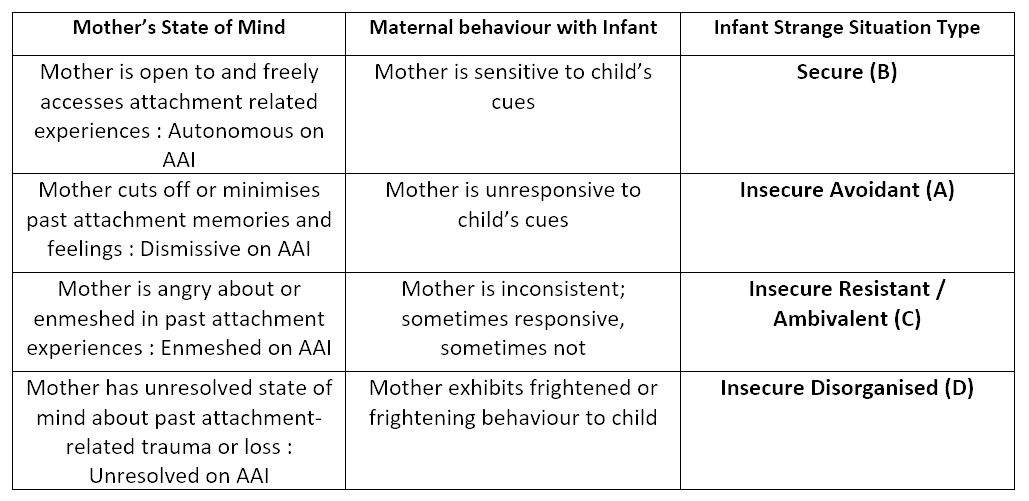
TABLE C. Hypothesised relationships between maternal stage of mind (from the AAI – Adult Attachment Interview), maternal behaviour, and child attachment type
Van Ijzendoorn (1995) looked at a large number of available studies in the decade since Main’s work and found considerable linkage between adult AAI (Adult Attachment Interview) and infant Strange Situation coding; Van Ijzendoorn argued that this “intergenerational transmission” of attachment may be via parent responsiveness and sensitivity. We discussed above how this is only a partial explanation, and other aspects of maternal behaviour and of the home environment may also be involved.
We have considerable evidence for some degree of continuity of attachment security through life, and onto the next generation; but considerable evidence that this can be affected by life events. An adult’s attachment security can also be influenced by counselling, clinical treatment, or simply by reflection [self mind-mindedness].
Some insight into this matter comes from a study by Fonagy et al. (1994). In a longitudinal study with 100 mothers and 100 fathers in London, who are given the AAI and other measures shortly before their child was born. The strange situation was used subsequently to measure security of attachment, to mother at 12 months and the father at 18 months. As many other studies have discovered, the parent’s AAI scores predicted the Strange Situation scores of the infants. The researchers also calculated the estimates of the amount of disrupted parenting and deprivation which the parents had experienced themselves, and use the measures to find out if these influenced infant attachment, which they did. However, the amount of disrupted parenting and deprivation the parents had experienced interacted strongly with the way in which the parents had dealt with their own representations of their experiences of being parented. Coding the AAI (Adult Attachment Interview), the researchers developed a Reflective Self-function scale to assess the ability parents had to reflect on conscious and unconscious psychological states, and conflicting beliefs and desires. Of 17 mothers with deprived parenting and low reflecting self-function scores, 16 had insecurely attached infants, as might have been expected. Completely opposite to this scenario 10 mothers who had experienced deprived but had high reflective self-function scores, all had securely infants. It was argued that reflective self-function could have the saliency to change the internal working models of people, and also demonstrate resilience to adversity and a way of breaking the inter-generational transmission of insecure attachment.
Adults who experienced difficult childhoods but have overcome early adversity and insecure attachment by a process of reflection, counselling or clinical help, are known as “earned secures”, and could be distinguished from “continuous secures”, who had a positive upbringing and what most might quality as “normal” childhood. Phelps et al. (1998) made home observations of mothers and their 27-month-old children, and found that earned-secures, like continuous secures, showed positive parenting; under conditions of stress, both these groups showed more positive parenting than insecure mothers.
Another fascinating perspective on this issue of inter-generational transmission of insecure attachments would be the Holocaust study (Bar-On et al., 1998; van Ijzendoorn et al., 1999). The Holocaust refers to the experiences of Jews and other persecuted unwanted & unassimilated minorities [who did not want to be Germans] in the concentration camps of World War II to be securely offloaded/deported when Adolf Hitler’s Germany became the Third Reich and when the policies changed to focus on National Socialism and Imperial Intentions of Expansion and Conquest (1939-45).

Jew Children: Here we see Jew school children in 1942. They look like younger children who are just beginning school. Notice that at least 2 teachers are with them. By this time the Jewish children had been forced out of public schools. For a short time however, they we allowed to attend schools set up by the Jewish community. At the time this photograph was taken, the transports to the deportation camps had already begun. Often children under 10-years of age were not required to wear the badges, but some of these children look much younger.
Although many revisionist such as the English historian, David Irving, of this dark part of human history are finding out inaccuracies regarding the true people responsible for those massacres [since no evidence has been found of Hitler giving any extermination order] along with other atrocities as evil if not worse than the deaths in concentration camps [for a section of a population that was causing instability to the proper functioning of a nation during times of revolt and huge global conflicts involving economic treaties, Jewish propaganda and ultra-liberal communist migration agendas fused with policies based on business & banking motives] committed by many of the “supposed good guys of the Allies” that involved the rape and murder of innocent children and women, fuelled by pure hate, Bolshevism and Jewish Communism against the native aryans of Germany [i.e. the German Volk/People].
A documentary extract from the diary of Dr. Joseph Goebbels who decided to take a firm stance against the national destruction of Germany (and Western Europe), Christianity, and whom many Nationally oriented thinkers consider to be among the bravest of the last great Christian Aryan men to have walked the earth. [See Aryan Race et aussi Race Aryenne / Also to be noted perhaps quite surprisingly that there were strong ancient Aryan religious & mythological warrior values embedded in the mind of Heinrich Himmler (the Reichsführer of the SS), the person believed to have taken the decision to exterminate the jews (remember the term itself originated from human sacrifices by Jews to their god, Baal), as he told his personal masseur & physician Felix Kersten that he always carried with him a copy of the ancient Aryan scripture, the Bhagavad Gita because it relieved him of guilt about what he was doing – he felt that like the sacred warrior Arjuna, who was simply doing his duty for his people and their future without attachment to his actions]
But, since the majority on this planet have been made to believe one version where all the Jews and the alien army of the allies are the good guys, and all the Germans [including Adolf Hitler] were the blood-sucking vampires who also turned into cannibals on the week ends, we are going to base our comments on this politically correct version that the history books and mainstream publishers prefer. [Politics too nowadays is in serious need of revision; are people really divided into 3 main categories? Left, Centre and Right? I tend to believe that we are above all this and have elements of all 3 embedded in us as modern human beings of the 21st century]

Pigs of Democracy from George Orwell’s “Animal Farm” animation (1954) / « La Ferme des Animaux » de George Orwell (1954) / Orwellians still find inspiration from the story as can be seen from this Trump-like pig creature published recently on Mediapart | [NOTE: The full movie can be viewed here]
But getting back to the Bedouin cultured civilisation’s distinguished members, i.e. Jews as an example of victims in those concentration camps [that many people have begun to question the evidence used to claims of gas chambers (with a great amount found on territories occupied by Stalin) with many camp detainees reporting being kept in facilities with swimming pools, orchestras and kitchens, the number of casualties, and the true perpetrator of the crimes]. It is believed by most people of the 21st century who have had no other options but to take in their news from mainstream Jewish-owned media, that besides being treated like despicable rats, degraded and tortured, many of the Jews to be deported kept in those camps were killed [some shot like parasitic animals as they tried to escape], leaving behind them orphaned children in traumatic circumstances.
Our question here however in regards to the focal point of this section, i.e. “insecure attachments”, is whether such traumatic experiences could have an impact on attachment, and could this also have been transmitted inter-generationally to the Jewish children scattered around the globe today like modern gypsies? This issue of inter-generational transmission of insecure attachments is the focus of the Holocaust study (Bar-On et al., 1998; van Ijzendoorn et al., 1999). The study we are looking at encompasses 3 generations of Jews, now grandparents, who went through the Holocaust [note that the name Holocaust itself comes from an event involving human sacrifices to the Jewish god, Baal], typically as children themselves who had lost their parents; their children, now parents; and their grandchildren. These generations are compared here with comparable 3-generation families who had not experienced the Holocaust.
It was found that the effects of the Holocaust were evident in the grandparent generations, who showed distinctive patterns on the AAI (Adult Attachment Interview), scoring high on Unresolved, as would have been predicted, and high on unusual beliefs – another predicted effect of trauma and unresolved attachment issues. They also displayed avoidance of the Holocaust topic; a very common finding was that the experiences had been so horrific and disgusting that they were unable to talk about their experiences with their own offspring.
However, inter-generational transmission of attachment type was quite low for this group of Jews. The Holocaust parents (‘children of the Holocaust’) showed rather small differences from controls, scoring just slightly higher on Unresolved on the AAI. This normalization process continued to the next generation (‘grandchildren of the Holocaust’), for whom no significant differences in attachment were found from controls. This seems to suggest a minor trend of “Unresolved” attachment among these Jews [note that this is linked to Disorganised attachment in infants and today some question whether Type-B Securely attached infants are really the “Best” way to be, and whether other personality characteristics also help shape the individual’s uniqueness throughout life, such as their reflective abilities and internal working models (reshaped by other meaningful events/relationships) – however it is also important to note that attachment types are known to remain and be transmitted over generations for the majority of people with low self-reflective skills and intelligence].
Disorganised Attachment and Unresolved Attachment Representation
The pattern of infant attachment classed as “Disorganised” from the Strange Situation procedure, was only acknowledged much later than the other well known attachment types [Secure, Inscure Avoidant & Insecure Resistant/Ambivalent], and appears to have rather distinctive correlates.
It has been noted that Disorganised infants may show stereotypic behaviours such as freezing, or hair-pulling; contradictory behaviour such as avoiding the caregiver [e.g. mother] despite experiencing severe distress on separation; and also misdirected behaviour such as seeking proximity to the stranger instead of the caregiver. These characteristic behaviours are known as signs of Unresolved stress and anxiety, and for these types of infants the caregiver is a source of fright rather than a symbol of safety (See Table C) – (see Vondra and Barnett, 1999, for a collection of recent research).
Van Ijzendoorn, Schuengel and Bakermans-Kranenburg (1999) reviewed a series of studies on Disorganized attachment, and argued that it was mainly caused by environmental factors [i.e. exposure]; although there is also some evidence for genetic factors in Disorganised infant attachment, and it is known to be higher in infants with severe neurological abnormalities [e.g. cerebral palsy, autism, Down’s syndrome] – around 35%, compared with around 15% in normal samples. However, Type-D (Disorganised Attachment) is also especially for mothers with alcohol or drug abuse problems (43%) or who have maltreated or abused their infants (48%). Type-D attachment is not higher in infants with physical disabilities; and it is not strongly related to maternal sensitivity as such, however there is evidence relating it to maternal unresolved loss or trauma [like the Jews of the Holocaust generation as mentioned above].
While the Maternal Sensitivity Hypothesis suggests that maternal (in)sensitivity predicts secure (B) or insecure (A,C) attachment, a different hypothesis has been proposed to explain Disorganised Type-D attachment (See Table C), which is that it is would be the result from frightened or frightening behaviour by the caregiver (generally the mother) to the infant, resulting from the mother’s own unresolved mental state related to attachment issues [e.g. abuse by her own parent; violent death of a parent/or close one; sudden loss of a child].
A study in London by Hughes et al. (2001) compared the Unresolved scores on the AAI (Adult Attachment Interview) for 53 mothers who had infants born next after still birth, with 53 controls [normal mothers], and found out that among the mothers who had previously stillborn infants, 58% scored as Unresolved, compared to 8% of Controls; furthermore, 36% had Disorganised (Type D) infants, compared with 13% of controls. A statistical path analysis [looking at the relationships among all the variables showed that the stillbirth experience predicted Unresolved maternal state of mind, and that it was this variable [i.e. Unresolved state of mind] then predicted infant disorganisation.
The hypothesised behavioural aspects of maternal unresolved state of mind [and Disorganisation in infants] were supported by the study in Mali reported above. A study in Germany by Jacobsen et al. (2000) provided further support in which 33 children were examined along with their mothers at 6 years of age. Disorganised attachment (assessed from a reunion episode) was significantly related to high levels of maternal expressed emotion, defined as speech to the child that was severely critical of them or over-involved with them.
Van Ijzendoorn et al., (1999), in a review, also found that insecure Disorganised (Type D) attachment in infants predicted later aggressive behaviour, and child psychopathology. Carlson (1998) found significant prediction from attachment disorganisation at 24 and 42 months, to child behaviour problems in preschool, elementary school and high school. Taking into consideration the prior links to parental maltreatment and abuse, it is highly likely that the Disorganised (Type D) attachment type will be found to be the most relevant aspect of attachment in understanding severely maladaptative or antisocial behaviour in later life.
Origins of the Insecure Disorganised State of Mind
The origins of insecure-disorganised (Type D) attachment is becoming an increasingly researched topic, and this may be due to the fact that early disorganisation (Type D) has been identified as a risk factor for later psychopathology (Fearon et al., 2010; van Ijzendoorn et al., 1999), with studies identifying a link between insecure-disorganised attachment in infancy and behavioural problems in later childhood (Lyons-Ruth et al., 1993; Munson et al., 2001; Shaw et al., 1996).
In Main and Hesse’s (1990; Hesse & Main, 2000) their seminal work led to the argument that these insecure-disorganised (Type D) infants have not been able to establish an organised pattern of attachment because they have been frightened by the caregivers or have experienced their caregivers themselves showing fearful behaviour. This is supported by findings that have linked insecure-disorganised attachment to infant maltreatment or hostile caregiving (Carlson, Cicchetti, Brnett & Braunwald, 1989; Lyons-Ruth et al., 1991), maternal depression (Radke-Yarrow et al., 1995), and maternal histories of loss through separation, divorce and death (Lyons-Ruth et al., 1991).
In a meta-analytic review however, van Ijzendoorn et al. (1999) reported that 15% of infants in non-clinical middle class American samples are classified as insecure-disorganised (Type D), suggesting that pathological parenting practices cannot fully account for disorganised attachment in infants. As highlighted by Bernier and Mains (2008), the origins of attachment disorganisation are very complex, involving factors ranging from infants’ genetic make up to parents’ experiences of loss or abuse, and much remains to be learned about why some infants are unable to form and organised attachment relationship with the caregiver.
Links between Attachment & Emotional Development
It is fundamental to understand and grasp the importance of the early stages of life, as the brain’s cognitive patterns are shaped by these early experiences that tend to have a lasting effect on personality. The infant’s earliest mode of exploring and engaging with the world revolves around conveying emotions: fear, discomfort, pain, contentment, happiness.
As we have already explained above in the section exploring the reasons why infants develop particular attachment types, the caregiver’s responses [not sensitivity, but mind-mindedness, i.e. the ability to respond “appropriately” to the cues] to such emotional cues and their representations of their own childhood emotional experiences [generally measured with the AAI for Autonomous, Dismissing, Preoccupied or Unresolved] are accepted as strong predictors of attachment security [i.e. Autonomous – Secure, Dismissing –Avoidant, Preoccupied- Resistant and Unresolved – Disorganised].
With this in mind, it is quite surprising that so little research has been conducted on the relation between security and children’s emotional development.
There are 2 main ways in which links between attachment and emotional development have been addressed:
(i) The research has investigated whether infants’ early emotional experiences predict attachment security
(ii) The researchers have explored whether the security of the infant-caregiver attachment relationship predicts children’s subsequent emotional development.
Emotional Regulation and Attachment Security
This section is focussed mainly on how caregivers’ ways of responding to the infants’ emotional cues predict later attachment security.
Mothers of insecure-avoidant infants have been found to withdraw when their infants express negative emotions (Escher-Graeub & Grossmann, 1983). Conversely, mothers of insecure-resistant infants typically find it difficult to comfort their infants effectively, meaning that their responses result in prolonging their infants’ feelings of distress (Ainsworth et al., 1978).
Cassidy (1994) argued that caregivers may enable their children to develop good emotional coping and regulation strategies through their willingness to acknowledge and respond to their children’s emotions. She also argued that secure attachment is characterised by the openness with which the caregiver [mother, father, etc] recognises and discusses the full spectrum of emotions [which leads to the child’s understanding that emotions should not be supressed and can be dealt with effectively]. Insecure-avoidant attachment is generally associated with caregivers failing to respond to their infants’ negative emotions because of their tendency to bias interactions in favour of positive emotional expressions. On the opposite, insecure-resistant attachment is associated with the caregiver amplifying the infant’s negative affect. Cassidy maintained that mothers of insecure-resistant children fail to emphasise the importance of attachment relationships, and therefore adopt strategies that fail to help the child regulate negative emotion, hence, prolonging the need for contact with the mother [or caregiver].
Affect Attunement
Cassidy’s views are in synchronisation with other theoretical positions, such as Stern’s (1985) characterisation of sensitive parenting in terms of effect attunement, with the sensitive mother being the type of human being who is attuned to all of her infant’s emotions, is also accepting and sharing in their affective content.
Insensitive mothers on the other hand, undermatch or overmatch their infants’ emotional signals because of their own perceptual biases.
In support of these approaches, Pauli-Pott and Mertesacker’s (2009) investigation revealed that mismatches between maternal and infant affect at 4 months [e.g. mother shows positive affect while her infant demonstrates neutral or negative affect] predicted insecure mother-infant attachment at 18 months. Mind-mindedness is also operationalised in terms of the caregiver’s tendency to accurately interpret the infant’s cognitions and emotions, and has been found to predict later attachment security (Meins er al., 2001). Thus, observations by a mother of her infant displaying surprise in response to a jack-in-the-box, followed by enigmatic comments such as “my infant is surprised” are associated with subsequent secure attachment. In contrast, insecure attachment is related to mothers misreading their infants’ internal stress by, for example, commenting that the infant is scared when no cue to suggest such an emotion is present in the infant’s overt behaviour. In more recent work it has been found that these inappropriate mind-related comments are particularly common in mothers of insecure-resistant infants, with mothers in this group being more likely to comment inappropriately on their infants’ thoughts and feelings than their counterparts in the secure, insecure-avoidant and insecure-disorganised groups.
Evidence suggests that mothers in the insecure-avoidant and insecure-resistant groups are aware of over-controlling and under controlling strategies respectively in coping with their children’s negative emotions. Berlin and Cassidy (2003) followed up a sample of infants who had been assessed in the strange situation in infancy, and questioned the mothers when the children were aged 3 about how they dealt with their child’s emotional expressive, and found that insecure-Avoidant (Type A) group mothers reported the greatest control of their 3-year-olds’ negative emotional expressiveness [e.g. expression anger or fear], whereas mothers in the insecure-Resistant(Ambivalent – Type C) reported the least control of children of their children’s expressing negative emotions.
These findings suggest that maternal behaviours associated with avoidant and resistant attachment that have been observed in infancy are stable and persist into the preschool years.
Security-related differences in the way in which children regulate their emotions are also in line with Cassidy’s (1994) approach. Spangler and Grossman (1993) took physiological measures of infant distress during the strange situation procedure and compared these measures with infants’ outward shows of upset and negative affect. The physiological measures showed that insecure-Avoidant (Type A) group infants were as distressed or more distressed than their secured group conterparts (Type B), despite the absence of overt behavioural distress observed in the insecure-avoidant (Type A) groups infants. It was therefore concluded by Spangler and Grossman that insecure-Avoidant infants mask or dampen their expression of negative emotions as a way of coping with the facts that caregivers are likely to ignore or reject their bids for contact and comfort when they are distressed.
Belsky, Spritz, and Crnic (1996) reported that 3-year-olds who had been securely attached in infancy were more likely to recall and memorise the positive emotional events that had witnessed on a puppet show, whereas insecurely attached children tended to attend and remember only the negative events. On the same note, Kirsch and Cassidy (1997) found that both secure and insecure-resistant attachment in infancy were associated at 3 years of age with better remembering and recall for a story in which a mother responded sensitively to her child than to a story where the child was rejected.
In contrast to the scenario above, insecure-Avoidant infants showed no difference in their recall of the responsive versus rejecting stories. Kirsch and Cassidy also found that 3-year-olds classified as insecure in infancy were more likely than those in secure groups to look away from drawings depicting “mother” – child engagement.
These findings suggest that the positive experiences of secure infants with their caregivers may result in these children attending more to positive emotional events because they are consistent with their attachment security.
__________
(III) The Genetic/Psychosexual Model of Development (Sigmund Freud)
“For generations almost every branch of human knowledge will be enriched and illuminated by the imagination of Freud” (Jane Harrison, 1850- 1928)
The Genetic Model of Psychosexual Stages
The genetic model that we are now going to explore may not have much to do with genes, and relates more to the “development” of the child. Sigmund Freud proposed that childhood development proceeds through a series of distinct stages to adulthood, each of them with their own themes and preoccupations.
The stages are based on the life-drive present in all organisms, as Freud proposed, and it seems logical from a physician who carried empirical work on the sexual organs of eels, to assume that all organisms have the embedded urge for “life” [i.e the life drive to keep itself and its species alive, which involves sexual selection and the fertilisation achieved through sex] that is primarily sexual but some also argued that it can be interpreted (unconsciously or consciously) in other forms [as flamboyant French psychoanalyst, Jacques Lacan proposed in his Theory with the Symbolic, the Imaginary and the Real] to suit a sophisticated society [e.g. France] with all its dimensions. Freud proposed that the psychosexual stages are understood to be organised around the child’s emerging sexuality.
It is important however to not exaggerate or misinterpret Freud’s assumption and also to remember the logic and vital purpose behind the sexual (life) drive in organisms in its own existence and continuity [breeding]. This is also a very good discussion point for the 21st century as it seems to imply that all healthy organisms should have healthy sexual drives, but whether these should “always” find expression through genital sexual acts with another organism is debatable and questionable from an ethical and moral perspective [especially for those not in a healthy and stable relationship]; hence many psychologists recommend “masturbation” as a healthy and safe alternative in managing excessive sexual desires in both young people and adults.
In the process of the child’s emerging “sexuality”, the term “sexual drive” itself meant more than simply adult genital sexuality, and from a psychological perspective, was broadly referring to a physiological/biological sense of “pleasure in the body” and more to “sensuality”. As many psychologists who based their foundations on some aspects of Freudian perspectives, it is assumed that adult sexuality is nothing more than the simple culmination of an orderly set of steps in which the child’s “psychosexual” focus shifted from one part of the body to another, with these body parts or “erotogenic zones” all having something in common with the generation of pleasure; which are orifices lined with sensitive mucous membranes.
Hence, Sigmund Freud may have adequately proposed in a statement regarding mental health that, “the only unnatural sexual behaviour is none at all.”, taking note once again that the term “sexual” from a psychologist exploring the developmental stages of a child generally tends to refer more to “sensuality”. The erotogenic body parts with orifices and sensitive mucous membranes leads to the infant sensuality being initially centred on the mouth (oral cavity), followed by the anus and then the genitals in early childhood. After some characteristic drama at about the age of 5, the child’s sexuality goes nearly completely dormant for a few years, before re-emerging with a vengeance [a rush of hardly managed sexual feelings] when puberty hits.
As the tradition on the debate of the development of the mind itself as an entity [that reflects in linguistic form the desires, both conscious and unconscious of the human organism] goes on among psychologists in the quest for these answers, we are also familiar with critics [mostly from the reductionist schools of thoughts (e.g. Pavlovian) such as the cognitive-behavioural enthusiasts and the medical department with its accolade, the pharmaceutical industry] who have not been entirely positive about Freud’s contribution to knowledge and are still unconvinced [perhaps due to their philosophy on a kind of methodological epistemology that is lacking to cope with matters of the mind] about the unconscious part of the mind that plays a huge role in our conscious behaviour. This may not be completely negative to intellectuals who subscribe to a version of reality that is embedded in language since critics in many cases have led to systematic investigations [scientific methodology] and until now there is an increasing body of evidence that points to the existence of an unconscious drift/urge/motive that exists in all organisms [e.g. as we noted in the essay about Biological Constraints in Learning by Operant Conditioning and also other studies carried out on priming along with observations of the symptomatic manifestations of certain mental disorders such as OCD and Panic Attacks].
The psychoanalytic theory has been modified by some of the best minds of the psychoanalytic tradition [e.g. Jung, Lacan, and some components adopted by ourselves in the conception of the model of mental life within the Organic Theory] since Freud left the questions open with the freedom of dialogue over the concepts and their expansions and applications throughout various dimensions [e.g. analysing qualitative subjective experiences of the expression of love and passion, or the obsoleteness of politics in modern society, or the impact of animal studies in designing a human world]. However, between all the versions of Freud’s theories, there are 3 components that have never been denied by any great psychoanalyst, which are the 3 structures first mentioned in the early Topographic Model, that is, the Unconscious, the Subconscious and the Conscious. These were later replaced with the Structural Model, which is the popular version that remapped and renamed the concepts, and which includes the (unconscious) id [present in all new born infants which consists of impulses, emotions & desires – id demands instant gratification of all wishes and needs], the (conscious, me) ego [which acts a mediator between reality and the desires of the id] and the (subconscious) superego [the conscience: the sense of duty & responsibility], that adepts such as Jacques Lacan and Carl Jung rejected over the earlier Topographic model [being one that is more flexible for the development of further refined models that also have the option to define the life force in other ways than the questionable specificity of the Structural Model’s id, ego & superego.
The 5 Psychosexual Stages
Stage I: The Oral Stage (from birth to 1 year old approximately)
From Freudian assumptions, it is believed that the voracious sucking of infants is not pure nutritional, although the infant clearly has a basic need to feed, it also takes a “pleasure” in the act of feeding, a feeling that Freud did not hesitate to quality as sexual and perhaps more “sensual” at this stage as babies appear to enjoy the stimulation of the lips [in play] and the oral cavity, and will often happily engage in “non-nutritive sucking” when they are no longer hungry and the milk supply is withdrawn. Beyond being an intense source of bodily pleasure – an early expression of later sexuality – sucking also represents the infant’s way of expressing love for and dependency on its feeder [normally it is the mother, but it can also be a primary caregiver that the child is attached to, hence Lacan proposed that the Oedipal & Electra complexes may not only not be true for ALL cases, but the child’s early sexual feelings may be projected on other primary caregivers and not necessarily the direct parents]. The sucking behaviour also serves to a general stance that the infant takes towards the world, one of “incorporation” or the taking in of new experiences.
Stage II: The Anal Stage (1 to 3 years old approximately)
At the second stage, the Anal stage, the focus shifts from one end of the digestive tract to the other at it happens at around the age of 2, when the child is developing an increasing degree of autonomous control over its muscles, including the sphincters that control excretion. After the incorporative passivity and dependency of the oral stage, the child begins to take a more active approach to life [note the term active also in line with Jean Piaget’s views on the development of the human child]. Sigmund Freud proposed that these themes of activity, autonomy and control, play out most crucially around the anus as the child learns to control defecation, and learns that it can control its direct external environment, in particular its caregivers attention, by expelling or withholding faeces. Moreover, the child takes a sort of sadistic pleasure in this control, a form of pleasure described as “Anal erotism”. An important conflict for the child during this stage involves toilet training, with struggles/disapproval taking place over the parents/caregivers demand that the child control its defecation according to particular rules. However, the anal stage represents a set of themes, struggles, pleasures, and preoccupations that cannot be reduced in any simple way to toilet-training, as many common psychology students from the wrong linguistic vein are in caricatures of Freud maybe in a defensive act for their lack of linguistic subtlety to understand the mental life and the models that govern it.
Stage III: The Phallic Stage (3 to 6 years old approximately)
Gradually, although still in the early childhood years, the primary location of sexual pleasure and interest shifts from the anus to the genitals, where the little boy starts to become fascinated with his penis while his counterpart, the little girl on other side of the gender register, develops a fascination with her clitoris. However, this stage is known as “phallic” and not “genital” because Freud maintained that both sexes were focused on the male organ; “phallus” referring not to the actual physical organ, the anatomical penis, but to its “symbolic value”. Briefly explained, the phallic stage is set as the little boy understanding that he has the penis [which has a symbolic value] which the little girl lacks, and develops the belief that he could possibly lose it. In contrast, the little girl does not have a penis and wishes to have one.
This is the very first time that the difference between the sexes comes into play in childhood development, and the contrast between masculinity and feminity, really becomes an issue for the child. It is also the 1st stage at which Freud’s psychosexual theory recognises sexual differences, and marks the crucial point at which, children become gendered beings [between the ages of 3 – 6].
The little boy’s and the girl’s differing relation to the phallus [remember: the “symbolic value” of it not the actual organ] plays a vital role in unfolding drama that takes place within the family during this stage, somewhere around the age of 3 to 5. It has been dubbed the “Oedipus complex”, after the Greek legend in which Oedipus unwittingly murders his father and marries his mother, his original love-object [remember the attachment period in Bowlby’s along with breastfeeding] after all, as is consequently envious of his father, who seems to have his mother to himself. The boy’s fearful recognition that he could lose his penis [symbolically: “masculinity”] – “castration anxiety” – becomes focussed on the idea that the competing male for the love of the mother[the father], could inflict this punishment on him if the boy’s sexual feelings and desire for the female figure of the caregiving mother is recognised. So, faced with fear, he renounces and represses the sexual feelings and desire, to instead identity with the father, becoming his imitator rather than his rival. In this process, the boy learns about masculinity and internalises the societal rules and norms [e.g. about relationships] that the father represents [the development of the Super-Ego, a sense of duty and responsibility, i.e. “conscience” takes place as the Structural Model suggests].
In the case of the little girl, matters are slightly different, and the developing child soon feels her lack of a penis keenly (“penis envy”) and blames the mother for leaving her so grievously unequipped, and then the father soon turns into her primary love-object [the “Electra Complex” appears as the opposite of the “Oedipus” Complex], and the mother her rival.
A similar process to the little boy now takes place in the little girl’s realm, resulting in the repression of her sexual feeling, desires and love, to shift to an identification with her mother, and hence with feminity. However, given that the girl is not under any “castration” threat, this process occurs under much less emotional pressure than in the little boy’s case. Consequently, perhaps due to this difference in emotional pressure, Freud proposed that the Electra complex was resolved less conclusively and with much less complete repression in girls than in boys, but also that girls tend to internalise a conscience [preconscious, or superego] that is in some ways weaker and less prohibitive and punitive than boys. It is not surprising that such a controversial claim about girls has been highly criticised specially with no scientific evidence to back it up; and is perhaps also one reason why Freud’s account of Oedipal [Electra complex] conflict in women has been the subject of much revision [e.g. by Jacques Lacan].
Stage IV: Latency (6 years old to puberty)
After the upheavals of the Oedipus and Electra complexes, the sexual drives go into a prolonged “semi-hibernation”. During the pre-pubertal school years, children engage in much less sexual activity and their relationships with others are also desexualised. Instead of desiring the primary caregivers and original love-objects, their parents, children now begin to identify with them – having structured their understanding of the world. However, this sudden interruption of childhood sexuality is largely a result of the massive repression of sexual feelings that concluded the phallic stage. One of the main consequence of this repression is that children come to completely forget their earlier sexual feelings, a major source [Freud claimed] of our general amnesia for early childhood experiences. Other institutional settings with their own social models such as formal schooling, reinforce the repression of sexuality during latency, leading children to focus their energies instead on mastering “culturally valued” knowledge and skills. Freud observed that the desexualisation of latency-age children was less complete among so-called “primitive” peoples.
Stage V: The Genital Stage (from the onset of puberty to death)
The latency period of forced or socially imposed sexual repression ends with the biologically-driven surge of sexual energy that accompanies puberty. This marks the final stage of psychosexual development where it all the previous stages were successfully completed, leaves the person with the ability for mature love with sexual feelings. It is important to note that the focus on sexual pleasure is once more shifted to the genitals as it was before the stage of latency [during the phallic stage (3 – 6 years old)] however, now it is fused with the ability for sensible and true affection for the object of desire [and not simply immature sexual feelings trying to find expression from an inadequately developed brain being projected at the easiest accessible caregiver].
In addition, both sexes are now invested in their own genitals rather than sharing a focus on the “symbolic value” of the penis as it occurred during the “Phallic stage”. The Genital Stage therefore marks the end of the “polymorphous perversity” of childhood sexuality. However, these erotic moments have not completely vanished but are instead subordinated to genital sexuality, often finding expression in other subtle ways [e.g. sexual foreplay].
According to the genetic model of psychosexual stages, we pass through each of the psychosexual stages on the way to maturity. However, we do not pass through them unscathed, and there are many ways in which people have problematic difficulties in particular stages [unable to progress successfully] and when such incidents happen a “fixation” develops. A fixation is simply an unresolved difficulty involving the characteristic issues of the particular stage, and leads to a fault-line in our personality, according to Freudian developmental perspectives.
If the individual failed to receive proper and reliable nurturance and gratification during the oral stage – or alternatively if they were over-indulged – a fixation on that stage may develop. It is believed that when a person is confronted with some forms of stresses, they may revert to the typical immature ways of dealing with the world of that period [at the particular point in time of that stage], this process was referred to as “regression” by Freud.
In some cases, fixations may lead to full-fledged mental disorders: Oral fixations are linked to depression and addictions, anal fixations to obsessive-compulsive disorder, and phallic fixations to hysteria [in severe cases]. Fixations [generally later countered by Reaction Formation] do not simply represent forms of behaviour and thinking that people regress to when faced with difficulties but the whole personality [thought structure] or “character” – the term Freud preferred – may be organised around the themes of the stage at which the person is most strongly fixated. As a result, Freud proposed a set of distinct stage-based character types:
(i) Oral Characters
This category of characters tend to be marked by passivity and dependency [think of the sheep metaphor], and are liable to use relatively immature ego defences such as denial.
(ii) Anal Characters
Anal people tend to be inflexible, stingy, obstinate and orderly, with a preference for defence mechanisms such as the isolation of affect [hide their feelings] and reaction formation.
(iii) Phallic Characters
Phallic characters are generally impulsive, vain and headstrong [think alpha-male prototype] with a preference for a defensive style that favours repression.
It is important to note that this 3-part typology is the closest that the psychoanalytic theory of personality comes to bringing forward an explanation for individual differences in personality from early childhood experiences. A phase of development pivotal to the other 2 mentioned theories which also attribute the foundations of fundamental structures to the period of infancy and childhood, although they all also acknowledge the individual’s ability to shape their own minds and correct their own problematic traits through reflection, and indeed as mentioned in the section on John Bowlby’s theory of attachment mothers with high reflective abilities were able to reshape the internal working models of their children’s attachment style and subsequent emotional development. It is to also be noted how all these 3 theorists although different in their perspectives, have been inspired by each other’s works, the idea of attachment itself was inspired by Freud’s pre-oedipal claims, and Jean Piaget like Sigmund Freud came from the school of thought that viewed the mind as an “active” entity in its development and creation, and not a “passive” entity generated by a ball of soft matter acting like a junction box with scripts for stimuli.
Psychoanalysis, then and now
One of the main claims of Freudian theory is that much of what motivates us to move forward in life is determined by the unconscious, and since by the reductionist mind state of the common researcher who sadly only had empiricism to dream of a better life for himself, these unconscious processes cannot be measured [such as moles, weight, fingers, teeth, sheep, cattle, etc], and hence it is often claimed [without much understanding or linguistic abilities or skills in discourse and philosophy] that belief in Freudian ideas is precisely that – beliefs rather than mechanical models based on empirical evidence [e.g. medicine, physics, surgery, chemistry, biology, etc – all the disciplines of the hard sciences].
However, while Freud’s views are almost impossible to test with reductionist quantitative methods, his theories and claims have influenced many psychologists who work with different methodologies and the unconscious processes of the brain are also being backed up by emerging fields that focus on the physiology of the brain [e.g. cognitive-neuroscience].
To illustrate one of those views that are hard to test empirically, consider the Freudian notion of “Reaction Formation”. It is assumed for example that if an individual is harshly [by strict parents] toilet trained as a child then the Freudian prediction would be that the person becomes “anally retentive” [i.e. excessively neat and tidy]. However, if in some ways we do recognise such tendencies in ourselves [once again prompting to the existence of a well developed with reflective and perspective taking abilities fully developed by Piaget’s standards], maybe even unconsciously, then we may react against it [Reaction Formation occurs] and we actively become very untidy.
This suggests that we are in control of ourselves and we have the ability to reverse the effects of our upbringing and early childhood experiences, which means in turn that it is impossible to predict a child’s development despite the fact that the first 6 years from birth are supposedly critical in determining later personality formation [self-reflective people save themselves from the mediocrity of the masses].
Freudian Theory has been of immense importance in pointing out 2 possibilities. One is that early childhood can be immensely important in affecting and determining later development [a position also adopted by other major theorists as we have seen such as Bowlby], and the other is that we can be driven by unconscious needs and desires which we are not aware of [until exposed to the right environmental stimuli that release them from their hidden depths]. Thus, it is assumed that if we not complete one of the childhood psychosexual stages very well, it could reflect itself later in adult disorders such as neurotic symptoms, but we would not be aware of the source or cause of the problem. The only way to come to terms with these deeply embedded problems in the depth of the individual’s psyche that has more saliency than the minor cognitive schemas for basic environmental interactions [e.g. making a cup of tea or a sandwich], is through close intensive sessions of psychoanalysis (see Picture G) in which the analyst peers into the unconscious to try and unravel [discover] the problems that occurred during the patient’s childhood development that is causing the current problems.
PICTURE G. The psychoanalyst tries to uncover the childhood unresolved issues to find the causes of the current problems.
Whatever its weaknesses are, the psychoanalytic theory remains the most complete theory in terms of depth and detail in capturing the essence of the human mind [soul as metaphor, or psyche], and today there are still many who believe that psychoanalytic theories are fundamental in understanding human development with many theoreticians who have brought forward variations and alternatives to Freud’s proposals on some controversial issues [e.g. Jacques Lacan, John Bowlby and Carl Jung] while many of his proposals have also lead to the scientific discovery of unconscious mental processes.
_____________________________________
*****
Références
- Ainsworth, M.D.S. & Wittig, B.A. (1969). Attachment and exploratory behaviour of one year olds in a strange situation. In B.M. Foss (Ed.) Determinants of infant behaviour, vol. 4. New York: Barnes and Noble.
- Ainsworth, M.D.S. (1963). The development of infant-mother interaction among the Ganda. In B.M. Foss (Ed.) Determinants of infant behaviour (Vol. 2). London:Methuen; New York: Wiley.
- Ainsworth, M.D.S. (1967). Infancy in Uganda: Infant care and the growth of love. Baltimore, MD: Johns Hopkins University Press.
- Ainsworth, M.D.S., Bell, S.M. & Stayton, D.J. (1971). Individual differences in Strange Situation behaviour of one year olds. In H.R. Schaffer (Ed.) The origins of human social relations. New York: Academic Press.
- Ainsworth, M.D.S., Bell, S.M. & Stayton, D.J. (1974). Infant-mother attachment and social development: Socialisation as a product of reciprocal responsiveness to signals. In M.P.M. Richards (Ed.) The introduction of the child into a social world. London: Cambridge University Press.
- Ainsworth, M.D.S., Blehar, M.C., Waters, E. & Wall, S. (1978). Patterns of attachment: Assessed in the strange situation and at home. Hillsdale, N.J.: Lawrence Erlbaum.
- Anderson, J. W. (1972). Attachment behaviour out of doors. In N. Blurton Jones (ed.), Ethological Studies of Child Behaviour. Cambridge: Cambridge University Press.
- Anderson, S.W., Bechara, A., Damasio, H., Tranel, D., Damasio, A.R. (1999) Impairment of social and moral behaviour related to early damage in human prefrontal cortex. Nat Neurisci, 2(11), 1032-7
- Baillargeon, R and DeVos, J. (1991). Object permanence in young infants: further evidence. Child Development, 62, 1227-46.
- Bar-On, D., Eland, J., Kleber, R.J., Krell, R., Moore, Y., Sagi, A., Soriano, E., Suedfeld, P., van der Velden, P.G. & Van Ijzendoorn, M.H. (1998). Multigenerational perspectives on coping with the Holocaust experience: an attachment perspective for understanding the developmental sequelae of trauma across generations. International Journal of Behavioural Development, 22, 315-38.
- Belsky, J., Spritz, B. & Crnic, K. (1996). Infant attachment security and affective-cognitive information processing at age 3. Psychological Science, 7, 111-114.
- Berlin, L.J. & Cassidy, J. (2003). Mothers’ self-reported control of their preschool children’s emotional expressiveness: A longitudinal study of associations with infant-mother attachment and children’s emotion regulation. Social Development, 12, 477-495.
- Bernier, A. & Meins, E. (2008). A threshold approach to understanding the origins of attachment disorganisation. Developmental Psychology, 44, 969-982.
- Blakemore, S.J., Den Ouden, H., Choudhury, S., Frith, C. (2007). Adolescent development of the neural circuitry for thinking about intentions. Social Cognitive and Affective Neuroscience, 2(2), 130-9
- Bliss, J. (2010). Recollections of Jean Piaget. The Psychologist, 23, 444-446.
- Boden, M. A. (1979). London: Fontana.
- Borke, H. (1975). Piaget’s mountains revisited: Changes in the egocentric landscape. Developmental Psychology, 11, 240-3.
- Bower, T.G.R. (1982). Development in Infancy, 2nd San Francisco: W. H. Freeman
- Bowlby, J. (1958). The nature of child’s tie to his mother: International Journal of Psycho-Analysis, 41, 251-269.
- Bowlby, J. (1969 / 1982). Attachment and loss, vol. 1: Attachment(2nd) New York: Basic Books.
- Bowlby, J. (1988). A Secure Base: Clinical Applications of Attachment Theory. London: Routledge.
- Bretherton, I & Waters, E. (eds) (1985). Growing points of attachment theory and research. Monographs of the Society for Research in Child Development, 50, nos 1-2.
- Bronfenbrenner, U. (1979). The Ecology of Human Development. Cambridge, MA: Harvard University Press.
- Bryant, P. E. and Trabasso, T. (1971). Transitive inferences and memory in young children. Nature, 232, 456-8.
- Butler, M., Retzlaff, P., & Vanderploeg, R. (1991). Neuropsychological test usage. Professional Psychology: Research and Practice, 22, 510-512
- Carlson, E.A. (1998). A prospective longitudinal study of attachment disorganisation/disorientation. Child Development, 69, 1107-28.
- Cassidy, J. (1994). Emotion regulation: Influences of attachment relationships. In N. Fox (Ed.) The development of emotion regulation: Biological and behavioural constraints (pp. 228-250). Monographs of the Society for Research in Child Development, 59 (2-3, Serial No. 240).
- Cohen, L. J. & Campos, J. J. (1974). Father, mother and stranger as elicitors of attachment behaviour in infancy. Developmental Psychology, 10, 146-54.
- Danner, F. W. and Day, M. C. (1977). Eliciting normal operations. Child Development, 48, 1600-6.
- De Wolff, M.S & Van Ijzendoorn, M.H. (1997). Sensitivity and attachment: a meta-analysis on parental antecedents of infant attachment. Child Development, 68, 571-91.
- Demakis, G. J. (2003). A meta-analytic review of the sensitivity of the Wisconsin Card Sorting Test to frontal and lateralized frontal brain damage. Neuropsychology, 17, 255-264
- Diamond A. (2002). Normal development of prefrontal cortex from birth to young adulthood: cognitive functions, anatomy, and biochemistry. In: Stuss DT, Knight RT, editors. Principles of frontal lobe function. New York: Oxford University Press. P 466-503
- Donaldson, M. (1978). Children’s Minds. London: Fontana.
- Dozier, M., Stovall, K.C., Albus, K.E. & Bates, B. (2001). Attachment for infants in foster care: The role of caregiver state of mind. Child Development, 72, 1467-77.
- Eling, P., Derckx, K., & Maes, R. (2008). On the historical and conceptual background of the Wisconsin Card Sorting Test. Brain and Cognition, 67, 247-253
- Fearon, R.P., Bakermans-Kranenburg, M.J. & Van Ijzendoorn, M.J. (2010). The significance of insecure attachment and disorganisation in the development of children’s externalising behaviour: A meta-analytic study. Child Development, 81, 435-456.
- Fifer, W. (2010). Prenatal Development and risks. In G. Bremner & T. Wachs (Eds.), The Blackwell Handbook of Infant Development.Oxford: Wiley/Blackwell.
- Flavell, J.H. (1996). Piaget’s legacy. Psychological Science, 7, 200-203.
- Fonagy, P., Steele, H. & Steele, M. (1991). Maternal representations of attachment during pregnancy predict organisation of infant-mother attachment at one year of age. Child Development, 62, 891-905.
- Fonagy, P., Steele, M., Steele, H., Higgitt, A. & Target, M. (1994). The theory and practice and resilience. Journal of Child Psychology and Psychiatry, 35, no.2, 231-57.
- Fox, N. (1977). Attachment of Kibbutz infants to mother and metapelet. Child Development, 48, 1228-39.
- Fox, N., Kimmerly, N.L. and Schafer, W. D. (1991). Attachment to mother / Attachment to father: a meta-analysis. Child Development, 62, 210-25.
- Gestsdottir, S. & Lerner, R. M. (2008). Positive Development in Adolescence: The development and role of intentional self-regulation. Human Development, 51, 202-224.
- Giedd, J.N., Blumenthal, J., Jeffries, N.O., Castellanos, F.X., Liu, H., Zijdenbos, A., et al. (1999). Brain development during childhood and adolescence: a longitudinal MRI study. Nat Neurosci, 2, 861-863
- Ginsburg, H. and Opper, S. (1979). Piaget’s theory of intellectual development: An introduction. Englewood Cliffs, NJ: Prentice-Hall.
- Grant, D.A. and Berg, E.A. (1948). A Behavioural Analysis of Degree Impairment and Ease of Shifting to New Responses in Weigh-Type Card Sorting Problem. Journal of Experimental Psychology, 39, 404-411
- Grossman, K.E., Grossman, K., Huber, F. & Wartner, U. (1981). German children’s behaviour towards their mothers at 12 months and their fathers at 18 months in Ainsworth’s ‘strange situation’. International Journal of Behavioural Development, 4, 157-81.
- Gruber, H. & Vonèche, J.J. (1977). The Essential Piaget. London: Routledge & Kegan Paul.
- Heaton, R.K., Chelune, G.J., Talley, J.L., Kay, G.G., & Curtis, G. (1993). Wisconsin Card Sorting Test manual: Revised and expanded. Odessa, FL: Psychological Assessment Resources
- Hepper, P. (2007). Prenatal Development. In A. Slater & M. Lewis (Eds), Introduction to Infant Development (2nded; pp. 41-62). Oxford: Oxford University Press.
- Hughes, P., Turton, P., Hopper, E., McGauley, G.A. & Fonagy, P. (2001). Disorganised attachment behaviour among infants born subsequent to stillbirth. Journal of Child Psychology and Psychiatry, 52, 791-801.
- Inhelder, B. and Piaget, J. (1958). The growth of logical thinking from Childhood to Adolescence. London: Routledge & Kegan Paul.
- Jacobsen, T., Hibbs, E. and Ziegenhain, U. (2000). Maternal expressed emotion related to attachment disorganisation in early childhood: a preliminary report. Journal of Child Psychology and Psychiatry, 41, 899-906.
- Jahoda, G. (1983). European ‘lag’ in the development of an economic concept: a study in Zimbabwe. British Journal of Developmental Psychology, 1, 113-20.
- Kirsch, S.J. & Cassidy, J. (1997). Preschoolers’ attention to and memory for attachment-relevant information. Child Development, 68, 1143-1153.
- Kochanska, G. (2001). Emotional development in children with different attachment histories: the first three years. Child Development, 72, 474-90.
- Levine, L.V., Tuber, S.B., Slade, H. & Ward, M.J. (1991). Mothers’ mental representations and their relationship to mother-infant attachment. Bulletin of the Menninger Clinic, 55, 454-469.
- Lewis, M., Feiring, C. & Rosenthal, S. (2000). Attachment over time. Child Development, 71, 707-20.
- Lewis, M., Feiring, C., McGuffoy, C. and Jaskir, J. (1984). Predicting psychopathology in six-year-olds from early social relations. Child Development, 55, 123-36.
- Lhermitte, F. (1983) “Utilization Behaviour” and its relation to lesions of the frontal lobes. Brain, 106, 237-255
- Lyons-Ruth, K., Alpern, L. & Repacholi, B. (1993). Disorganised infant attachment classification and maternal psychosocial problems as predictors of hostile-aggressive behaviour in the pre-school classroom. Child Development, 64, 527-585.
- Lyons-Ruth, K., Repacholi, B., McLeod, S. & Silva, E. (1991). Disorganised attachment behaviour in infancy: Short-term stability, maternal and infant correlates and risk-related subtypes. Development and Psychopathology, 3, 377-396.
- Main, M & Solomon, J. (1990). Procedures for identifying infants as disorganised / disoriented during the Ainsworth Strange Situation. In M.T. Greenberg, D. Cicchetti & E.M. Cummings (Eds.) Atttachment in the preschool years (pp. 121-160). Chicago; University of Chicago Press.
- Main, M. & Hesse, E. (1990). Parents’ unresolved traumatic experiences are related to infant disorganised attachment status: Is frightened and/or frightening parental behaviour the linking mechanism? In M.T. Greenberg, D. Cicchetti, & E.M. Cummings (Eds.) Attachment in the preschool years (pp.161-182). Chicago: University of Chicago Press.
- Main, M. & Solomon, J. (1986). Discovery of a disorganised/disoriented attachment pattern. In T.B. Brazelton & M.W. Yogman (Eds.) Affective Development in Infancy. Norwood, NJ: Ablex.
- Main, M., Kaplan, N. & Cassidy, J. (1985). Security in infancy, childhood, and adulthood: a move to the level of representation. In I. Bretherton and E. Waters (eds), Growing Points of Attachment Theory and Research. Monographs of the Society for Research in Child Development, 50, nos 1-2.
- Martorano, S. C. (1977). A developmental analysis of performance on Piaget’s formal operations tasks. Developmental Psychology, 13, 666-72.
- Masangkay, Z.S., McCluskey, K.A., McIntyre, C. W., Sims-Knight, J., Vaughn, B. E. and Flavell, J.H. (1974). The early development of inferences about the visual percepts of others. Child Development, 45, 237-46.
- McGarrigle, J. and Donaldson, M. (1974). Conservation accidents. Cognition, 3, 341-50.
- Meins, E., Fernyhough, C., Fradley, E. & Tuckey, M. (2001). Rethinking maternal sensitivity: Mothers’ comments on infants’ mental processes predict security of attachment at 12 months. Journal of Child Psychology and Psychiatry, 42, 637-648.
- Melhuish, E. (1993). A measure of love? An overview of the assessment of attachment. ACPP Review & Newsletter, 15, 269-75.
- Meltzoff, A and Moore, M. (1983). Newborn infants imitate adult facial gestures. Child Development, 54, 702-9.
- Meltzoff, A.N and Moore, M. K. (1989). Imitation in newborn infants: exploring the range of gestures imitated and the underlying mechanisms. Development Psychology, 25, 954-62.
- Miller P, Wang XJ (2006) Inhibitory control by an integral feedback signal in prefrontal cortex: A model of discrimination between sequential stimuli. Proc Natl Acad Sci USA, 103(1), 201-206
- Miller, P.H. (1993). Theories of Developmental Psychology (3rd edn). Englewood Cliffs, NJ: Prentice-Hall.
- Miyake, K., Chen, S.J. and Campos, J.J. (1985). Infant temperament, mother’s mode of interaction and attachment in Japan: an interim report. In I. Bretherton and E. Waters (eds), Growing Points of Attachment Theory and Research. Monographs of the Society for Research in Child Development, 50, 276-97.
- Norman, D.A., & Shallice, T. (1986). Attention to action: Willed and automatic control of behaviour. (Center for Human Information Processing Technical Report No. 99, rev. ed.) In R.J. Davidson, G.E. Schartz, & D. Shapiro (Eds.), Consciousness and self-regulation: Advances in research, (pp. 1-18). New York: Plenum Press
- O’Connor, T.G. & Croft, C.M. (2001). A twin study of attachment in preschool children. Child Development, 72, 1501-11.
- Oppenheim, D., Sagi, A. and Lamb, M.E. (1988). Infant-adult attachments on the kibbutz and their relation to socioemotional development 4 years later. Developmental Psychology, 24, 427-33.
- Pauli-Pott, U. & Mertesacker, B. (2009). Affect expression in mother-infant interaction and subsequent attachment development. Infant Behaviour and Development, 32, 208-215.
- Phelps, J.L., Belsky, J. & Crnic, K. (1998). Earned security, daily stress and parenting: a comparison of five alternative models. Development and Psychopathology,10, 21-38.
- Piaget, J and Inhelder, B. (1956). The Child’s Conception of Space. London: Routledge & Kegan Paul.
- Piaget, J. (1929). The Child’s Conception of the World. New York: Harcourt Brace Jovanovich.
- Piaget, J. (1936/1952). The Origin of Intelligence in the Child. London: Routledge & Kegan Paul.
- Piaget, J. (1951). Play, Dreams and Imitation in Childhood. London: Routledge & Kegan Paul.
- Piaget, J. (1955). The child’s construction of reality. London: Routledge and Kegan Paul.
- Radke-Yarrow, M., McCann, K., DeMulder, E., Belmont, B., Martinez, P. & Richardson, D.T. (1995). Attachment in the context of high-risk conditions. Development and Psychopathology, 7, 247-265.
- Rothbaum, F., Weisz, J., Pott, M., Miyake, K. & Morelli, G. (2000). Attachment and culture: security in the United States and Japan. American Psychologist, 55, 1093-105.
- Schaffer, H. R. (1996). Social Development. Oxford: Blackwell Publishers.
- Schaffer, H.R. & Emerson, P.E. (1964). The development of social attachments in infancy. Monographs of the Society for Research in Child Development,
- Shayer, M. and Wylam, H. (1978). The distribution of Piagetian stages of thinking in British middle and secondary school children: II. British Journal of Educational Psychology, 48, 62-70.
- Shayer, M., Kuchemann, D.E. and Wylam, H. (1976). The distribution of Piagetian stages of thinking in British middle and secondary school children. British Journal of Educational Psychology, 46, 164-73.
- Slater, A. & Bremner, G. (2011). An Introduction to Developmental Psychology (2nd). Oxford: Blackwell.
- Smith, P. K., Cowie, H. & Blades, M. (2003). Understanding Children’s Development. Oxford: Blackwell.
- Smith, P., Cowie, H. and Blades, M. (2003). Understanding children’s development. 4th ed. pp.388-416.
- Sowell ER, Thompson PM, Holmes C.J., Jernigan, T.L., Toga A.W. (1999). In vivo evidence for post-adolescent brain maturation in frontal and striatal regions. Nat Neurosci, 2, 859-861
- Spangler, G. & Grossman, K.E. (1993). Biobehavioural organisation in securely and insecurely attached infants. Child Development, 64, 1439-1450.
- Stern, D.N. (1985). The interpersonal world of the infant: A view from psychoanalysis and developmental psychology. New York:Basic.
- Stevenson-Hinde, J. & Verschueren, K. (2002). Attachment in childhood. In P.K. Smith and C.H. Hard (eds), Blackwell Handbook of Childhood Social Development. Oxford: Blackwell.
- Sylvia, K. & Lunt, I. (1981). Child Development: an Introductory Text. Oxford: Basil Blackwell.
- Takahashi, K. (1990). Are the key assumptions of the ‘strange situation’ procedure universal? A view from Japanese research. Human Development, 33, 23-30.
- True, M.M., Pisani, L. & Oumar, F. (2001). Infant-mother attachment among the Dogon of Mali. Child Development, 72, 1451-66.
- Van Ijzendoorn, M.H & Kroonenberg, P.M. (1988). Cross-cultural patterns of attachment: a meta-analysis of the Strange Situation Child Development, 59, 147-56.
- Van Ijzendoorn, M.H. & De Wolff, M.S. (1997). In search of the absent father – meta-analyses of infant-father attachment: a rejoinder to our discussants. Child Development, 68, 604-9.
- Van Ijzendoorn, M.H. (1995). Adult attachment representations, parental responsiveness, and infant attachment: A meta-analysis on the predictive validity of the Adult Attachment Interview. Psychological Bulletin, 117, 1-17.
- Van Ijzendoorn, M.H., Moran, G., Belsky, J., Pederson, D., Bakermans-Kranenburg, M.J. and Kneppers, K. (2000). The similarity of siblings’ attachment to their mother. Child Development, 71, 1086-98.
- Van Ijzendoorn, M.H., Sagi, A. & Grossman, K.I. (1999). Transmission of holocaust experiences across three generations Symposium presentation at IXth European Conference on Developmental Psychology, Spetses, Greece, 3 September.
- Van Ijzendoorn, M.H., Schuengel, C. & Bakermans-Kranenburg, M.J. (1999). Disorganised attachment in early childhood: meta-analysis of precursors, concomitants, and sequelae. Development and Psychopathology, 11, 225-49.
- Vondra, J.I. & Barnett, D. (1999). Atypical attachment in infancy and early childhood among children at developmental risk. Monographs of the Society for Research in Child Development, 64(3), serial no. 258.
- Waters, E., Hamilton, C.E. & Weinfeld, N.S. (2000). The stability of attachment security from infancy to adolescence and early adulthood: general introduction. Child Development, 71, 678-83.
- Waters, E., Vaughn, B.E., Posada, G. and Kondo-Ikemura, K. (1995). Caregiving, cultural and cognitive perspectives on secure-base behaviour and working models. Monographs of the Society for Research in Child Development, 60, nos 2-3.
- Weinraub, M. & Lewis, M. (1977). The determinants of children’s responses to separation. Monographs of the Society for Research in Child Development, 42, 1-78.
- Weisner, T.S. & Gallimore, R. (1977). My brother’s keeper: child and sibling caretaking. Current Anthropology, 18, 169-90.
- Willatts, P. (1989). Development of problem solving in infancy. In A. Slater and G. Bremner (eds), Infant Development. Hillsdale, NJ: Lawrence Erlbaum
- Wimmer, H. and Perner, J. (1983). Beliefs about beliefs: representations and constraining function of wrong beliefs in young children’s understanding of deception. Cognition, 13, 103-28.
Danny d’Purb | DPURB.com
____________________________________________________
While the aim of the community at dpurb.com has been & will always be to focus on a modern & progressive culture, human progress, scientific research, philosophical advancement & a future in harmony with our natural environment; the tireless efforts in researching & providing our valued audience the latest & finest information in various fields unfortunately takes its toll on our very human admins, who along with the time sacrificed & the pleasure of contributing in advancing our world through sensitive discussions & progressive ideas, have to deal with the stresses that test even the toughest of minds. Your valued support would ensure our work remains at its standards and remind our admins that their efforts are appreciated while also allowing you to take pride in our journey towards an enlightened human civilization. Your support would benefit a cause that focuses on mankind, current & future generations.
Thank you once again for your time.
Please feel free to support us by considering a donation.
Sincerely,
The Team @ dpurb.com
P.S.
– If you are a group/organization or individual looking for consultancy services, email: info[AT]dpurb.com
– If you need to reach Danny J. D’Purb directly for any other queries or questions, email: danny[AT]dpurb.com [Inbox checked periodically / Responses may take up to 20 days or more depending on his schedule]
Stay connected by linking up with us on Facebook and Twitter