
Mis à jour le Dimanche, 12 Décembre 2021

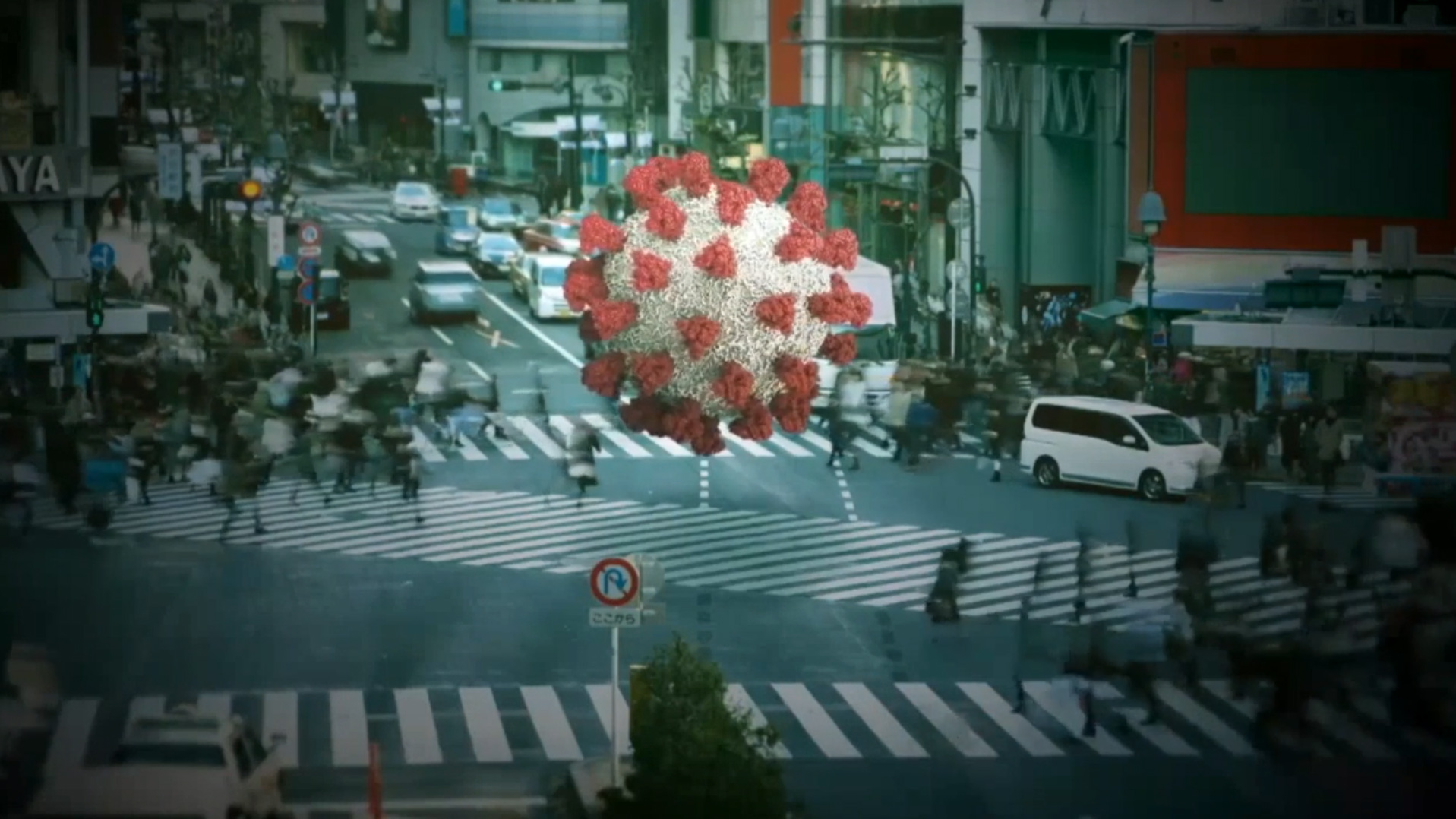
What we now know about the ugly SARS-CoV-2 virus is that it is among a group of coronaviruses that causes diseases in animals and birds, and respiratory tract infections in humans. These infections tend to be mild, but in rarer forms such as the Middle East respiratory syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) they can be fatal. SARS-CoV-2 shares a similar sequencing identity with the infamous SARS coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV), but SARS-CoV-2 is relatively more infectious in comparison to other CoV. SARS-CoV-2, SARS-CoV, and MERS-CoV are all suspected of being from animal reservoirs and then transmitted to humans.
The current outbreak declared by the World Health Organization (WHO) is caused by SARS-CoV-2 which has a close genetic similarity to bat coronaviruses and are thought to have been its likely origin. The virus primarily targets the respiratory system and causes flu-like symptoms upon exposure, although some patients may appear asymptomatic. In the early stages, the disease presents itself as a mild respiratory infection. However, as the disease progresses in severity, it may lead to acute respiratory failure, severe complications such as multiorgan failure, and ultimately death.
The wild tornado in the body: how the infection starts and kills
COVID-19 spreads in a similar way to cold and flu bugs; through droplets being left on surfaces after a person coughs or sneezes, which are then touched by other people and spread further. The Coronavirus (SARS-CoV-2 / CoVID-19) has been killing thousands of people every hour globally since it appeared. Clinicians and pathologists are still trying to fully understand how it inflicts such damage as it tears through the human body.
Although it well known that the lungs are ground zero (i.e. the main point of impact), the virus can extend to many other organs including the heart and blood vessels, kidneys, guts and brain. « Its ferocity is breathtaking and humbling », said Krumholz a cardiologist from Yale university.
The infection begins when an infected subject expels virus-laden droplets and another person inhales them, the SARS-CoV-2 coronavirus then enters the nose and throat and finds a comfortable home in the lining of the nose according to scientists from the Wellcome Sanger Institute. This region is lined with cell-surface receptor known as ACE2 (i.e. Angiotensin-converting enzyme 2) which are present throughout the body to help regulate blood pressure but it also marks tissues vulnerable to infection. The virus requires this receptor to enter a cell, and once inside it hijacks the cell’s machinery, multiplies itself and takes over new cells.
During the period where the virus is multiplying itself, an infected person may shed copious amounts of it, especially during the first week. There may not be any symptoms at this point, or the victim may develop a fever, dry cough, sore throat, loss of smell and taste, or head and body aches. If the immune system does not destroy the virus at this early stage, then it moves down the windpipe and starts to wreck havoc in the lungs where it can become deadly.
The thinner, distant branches of the lungs respiratory tree end in tiny air sacs called alveoli [alveolus (single)], each lined by a single layer of cells that are also rich in ACE2 receptors, the very same receptors that allows the virus to penetrate. When we are in good health, oxygen crosses the alveoli into the capillaries, which are tiny blood vessels that lie beside the air sacs (alveoli). That oxygen is then transported to the other regions of our body. But, when the immune system is stressed and fighting ardently against the virus, the battle disrupts the oxygen transfer. The front-line white blood cells release inflammatory molecules called chemokines, which in turn create more immune cells that target and destroy virus-infected cells. When these infected cells are destroyed by the chemokines, they leave a stew of fluid and dead cells – pus – behind. This process is the scenario that takes places in pneumonia and the corresponding symptoms are: coughing; fever; and fast, shallow breathing. In some cases, we find COVID-19 patients who recover, sometimes simply with oxygen breathed in through nasal prongs.
However, in other unfortunate scenarios, patients often deteriorate suddenly to develop a condition referred to as acute respiratory distress syndrome (ARDS), where they struggle to breathe as the oxygen levels in their blood falls abruptly. On x-rays and computed tomography scans, the lungs of these patients are shown to be riddled with white opacities where instead healthy dark space [i.e. air] should be. These cases end up on ventilators and many die. Autopsies have shown their alveoli (air sacs) stuffed with fluid, white blood cells, mucus and the detritus of destroyed lung cells.

Image: The cross section shows immune cells crowding an inflamed alveolus (air sac) whose walls break down during attack by the virus causing reduced oxygen intake – patients cough, experience rising fever and breathing becomes difficult / Source: Wadman (2020)
Some clinicians found that the driving force that leads to severely ill patients’ downhill trajectory and death to be a disastrous overreaction of their own body’s immune system, a reaction referred to as a « cytokine storm » , which viral infections are known to trigger. Cytokines are chemical signaling molecules that guide a healthy immune response, however, in a cytokine storm, the level of cytokines rise beyond the level of what is needed, and hence this excessive rush [i.e. storm] of immune cells also start to attack and destroy healthy tissues – these individuals’ blood vessels leak, blood pressure drops, blood clots form, and catastrophic organ failure can follow.
Some studies (Chen et al., 2020) have demonstrated elevated levels of these inflammation-inducing cytokines (Huang et al., 2020) in the blood of hospitalised COVID-19 patients. Jamie Garfield, a pulmonologist who treats COVID-19 patients at the Temple University Hospital argues that the real morbidity and mortality of this disease is probably driven by this out of proportion inflammatory response of the human immune system to the virus. However, other medical professionals are not convinced. “There seems to have been a quick move to associate COVID-19 with these hyperinflammatory states. I haven’t really seen convincing data that that is the case,” said Joseph Levitt, a pulmonary critical care physician at the Stanford University School of Medicine. Levitt is also worried that efforts to develop several drugs to dampen the cytokine response could actually cause harm by suppressing the immune response that our body needs to fight off the virus.
We find different views among the academic community on this new virus. Others are viewing it from a completely different perspective, and are focusing on the heart and blood vessels, that they believe is playing a significant role in the rapid deterioration of some patients.
Tearing the heart
All the classic symptoms of a heart attack was observed in a 53-year-old Italian woman in Brescia along with signs in her electrocardiogram and high levels of blood marker suggesting damaged cardiac muscles. Further tests revealed cardiac swelling and scarring, and a left-ventricle – which is usually the powerhouse chamber of a human heart – so weak that only one-third of the normal amount of blood could be pumped. When doctors injected dye in her coronary arteries to look for what they believed to be a blockage that is usually associated with heart attacks, they found nothing. The next test carried out revealed that the culprit was in fact COVID-19.
It is still a mystery to academics how the virus attacks the heart and blood vessels but many preprints and scientific papers attest that such damage is common. A JAMA cardiology paper observed damages to the heart in nearly 20% of COVID-19 patients (Shi et al., 2020) out of 416 hospitalised patients in Wuhan, China. Another Wuhan study revealed that 44% of 36 patients admitted in ICU had arrhythmias, i.e. irregular heart beats (Wang et al., 2020).
What has been discovered, is that the disruption extends to blood itself. Among 184 COVID-19 patients in a Dutch ICU, 38% had blood that clotted abnormally, and about one-third already had clots (Klok et al., 2020). Blood clots are very dangerous since they can break apart and end up landing in the lungs, blocking vital arteries – a condition known as pulmonary embolism, which has killed many COVID-19 patients. Blood clots from arteries can also end up in the brain, causing stroke. Many COVID-19 patients have dramatically high levels of D-dimer, a byproduct of blood clots. Hence, it is very likely that blood clots have a major role in the disease severity and mortality with the COVID-19 pandemic.
Infection may also lead to the constriction of blood vessels. There are reports emerging of ischemia [i.e. an inadequate blood supply to an organ or part of the body, especially the heart muscles] in the fingers and toes – reduction in blood flow can cause swollen, painful digits and eventually tissue death. Blood vessels carry oxygen to various parts of our body, and when they become constricted problems will logically arise. In the lungs, the constriction of blood vessels may explain the reports of a very perplexing phenomenon seen in patients with pneumonia caused by COVID-19: some patients although having extremely low blood-oxygen levels are not gasping for breath. Since we are still uncovering the depths of the virus, one explanation may be that at some stages of the disease, the virus modifies the delicate balance of hormones that regulate blood pressure and constricts the blood vessels going to the lungs. Logically, constricted blood vessels will lead to oxygen uptake being impeded – this may be the cause of low blood-oxygen levels rather than clogged alveoli (air sacks) as explained above.
It is very important to take note that if COVID-19 targets blood vessels, it may explain why patients with pre-existing damage to those vessels, such as those with diabetes and high blood pressure, face a higher risk of serious disease. The recent data from the Centers for Disease Control and Prevention (CDC) on hospitalised patients in 14 US states found that bout one-third had chronic lung disease and nearly as many had diabetes and half had pre-existing high blood pressure (Garg et al., 2020). It has also been observed that there is a very low number of cases suffering from asthma and other respiratory diseases. The risk factors seem to be vascular: diabetes, obesity, age and hypertension. Academics are still in the dark regarding the causes of cardiovascular damage. Since the lining of the heart and blood vessels are rich in ACE2 receptors just like in the nose and the alveoli, it is possible that the virus may be directly targeting and attacking them. Another possibility for cardiovascular damage could be the lack of oxygen caused by a combination of factors: lack of oxygen, chaos in the lungs and damages to blood vessels. A cytokine storm unleashed by the immune system itself could also be responsible for damages to the heart as it does for other organs.
Destruction in multiple zones
While there is worldwide tension regarding the shortage of ventilators for failing lungs, less attention has been given to dialysis machines. Jennifer Frontera, a neurologist from New York University’s Langone Medical Center who has treated thousands of COVID-19 patients pointed out that if patients are not dying from lung failure, they are dying from renal failure. Hence, her hospital is developing dialysis protocols with different machines to support additional patients. As usual, the ACE2 receptors, a favoured penetrating site for the virus, is abundantly present in kidneys. Going by a preprint, 27% of 85 hospitalised patients in Wuhan had kidney failure (Li et al., 2020). Another report read 59% of nearly 200 hospitalised COVID-19 patients in China’s Hubei and Sichuan provinces had protein in their urine (Diao et al., 2020), and 44% had blood clot; both suggest that kidney damage took place. Patients with acute kidney injury (AKI), were more than five times as likely to die as COVID-19 patients without it, the same Chinese preprint reported.
“The lung is the primary battle zone. But a fraction of the virus possibly attacks the kidney. And as on the real battlefield, if two places are being attacked at the same time, each place gets worse,” says Hongbo Jia, a neuroscientist at the Chinese Academy of Sciences’s Suzhou Institute of Biomedical Engineering and Technology and a co-author of that study.
The electron micrographs from the autopsies of kidneys revealed viral particles (Diao et al., 2020), suggesting a direct viral attack. However, the kidney injury may also be a collateral damage caused by ventilators – that heighten the risk of kidney damage – as do some antiviral compounds such as remdesivir [which has been used experimentally in early COVID-19 patients]. The immune system’s cytokine storms may also severely reduce blood flow to the kidney and often causing fatal damage. Diabetes can also increase the chances of kidney injury. Hence people with chronic kidney diseases are at a higher risk for acute kidney injury.
Combo hits to the brain
Another range of symptoms in COVID-19 patients focus on the brain and the central nervous systems (Mao et al., 2020). Frontera says that neurologists are required to assess 5% to 10% of coronavirus patients at her hospital and believes that it may be a gross underestimate of the number of patients whose brains are struggling since many are sedated and on ventilators. Patients have suffered from brain inflammation, encephalitis (Moriguchi et al., 2020), with seizures and with a sympathetic storm [i.e. a hyper reaction of the sympathetic nervous system that causes seizure-like symptoms and is mostly observed after a traumatic brain injury]. Some COVID-19 patients even lose consciousness for a short amount of time while others suffer strokes. The loss of the sense of smell has also been widely reported. Frontera and others are asking themselves whether in some cases, infection depresses the brain stem reflex that senses oxygen starvation; this may provide an explanation to why despite dangerously low blood oxygen levels, patients are not gasping for air.
The former coronavirus behind the 2003 severe acute respiratory syndrome (SARS) epidemic – a cousin of COVID-19 – could infiltrate neurons and at times caused encephalitis. Since ACE2 receptors are present in the neural cortex and brain stem, the virus could interact with those receptors and penetrate the brain. In a case study in the International Journal of Infectious Diseases, a team of academics from Japan found traces of COVID-19 traces in the cerebrospinal fluid of a patient who developed meningitis and encephalitis, insinuating that COVID-19 can penetrate the central nervous system.

Image: Tissue damage in the brain (milky white areas shown by the arrows) as a result of encephalitis developed by a 58-year-old woman infected with COVID-19 / Source: (Poyiadji et al., 2020)
However, other factors could also be damaging the brain, such as a cytokine storm triggered by patients’ immune system itself, leading to swelling, and the blood’s exaggerated tendency to clot could trigger strokes. The collection of neurological data from care patients received is ongoing at a worldwide consortium that now include 50 centers in order to identify the prevalence of neurological complications in hospitalised COVID-19 patients and document how they fare.

The aim of course is to better understand the virus’ impact on the nervous system, including the brain. Sherry Chou, a neurologist speculates about an invasion route for the virus: through the nose, then upward through the olfactory bulb which connects to the brain, which may explain the loss of smell.
To the gut
Diarrhea with blood, vomiting and abdominal pain was reported in early March 2020 from a 71-year-old woman from Michigan who returned from a Nile river cruise. Doctors suspected the common stomach bug, e.g. Salmonella. However, after she developed a cough, nasal swabs revealed that she was positive for COVID-19. Gastrointestinal (GI) infection was diagnosed after a stool sample was positive for viral RNA and an endoscopy revealed signs of colon injury according to a paper in The American Journal of Gastroenterology (AJG) (Click to see).
This case adds to a growing body of evidence suggesting that like the SARS, COVID-19 can infect the lining of the lower digestive tract where, once again, the ACE2 receptors needed for the virus to enter are abundant. As many as 53% of sampled patients’ stool samples have shown to contain viral RNA. The virus’ protein shell was also found in gastric, duodenal and rectal cells in biopsies by a Chinese team who reported it in a paper in Gastroenterology (Xiao et al., 2020). “I think it probably does replicate in the gastrointestinal tract,” said Mary Estes, a virologist at Baylor College of Medicine.
Up to 50% of patients, making up about 20% across studies experience diarrhea. Gastrointestinal Infection (GI) however is not on the CDC’s list of COVID-19 symptoms which could lead to some COVID-19 cases to go undetected. The co-editor of Gastroenterology, Douglas Corley of Kaiser Permanente, Northern California said: “If you mainly have fever and diarrhea, you won’t be tested for COVID.”
So, can COVID-19 be passed on through feces? We do not know if the stool contains active, intact, infectious virus or simply RNA and proteins, there is no evidence to date. Based on experiments with SARS and with the virus that causes Middle East respiratory syndrome, a cousin of COVID-19, the risk from fecal transmission is probably low.
Finally, the virus also affects the eyes as one-third of hospitalised patients develop conjunctivitis – reddish, watery eyes – although it is not clear if the virus directly attacks the eyes (Wu et al., 2020). Some other reports have also suggested liver damage since more than 50% of COVID-19 (Zhang, Shi and Wang, 2020) patients hospitalised in two Chinese centers had elevated levels of enzymes (Fan et al., 2020) which suggest injury to the liver or bile ducts. However, many experts reportedly told Science that direct viral hits are unlikely, stating that other events in a failing body, like drugs or an immune system overdrive, are more likely driving the liver damage.
COVID-19 is a new virus and the academic community are only beginning to uncover its secrets and find answers to these questions:
Who is most vulnerable?
Why does it develop so rapidly and why it is so hard for some patients to recover?
Why does the infection spread so rapidly from people who are asymptomatic?
Why some patients are hardly affected while others are hit so severely?
The answers to those questions lie in the depths of our immune system. In the human body, immune cells are microscopic warriors that fight off invasive viruses in our body and we have 2 trillion of those. When viruses enter our body, immune cells instantly track them and devour the enemy, injecting toxins to destroy them and sometimes even release a sticky web to ensnare them.
Latest scientific discoveries are beginning to uncover the enigmatic mechanism behind our immunity. We are now confident that the novel coronavirus has the ability to break down our immune defences with its formidable powers; COVID-19 slips through, suppresses and unleashes chaos. Research on the human immune system is continuing and is helping to find potential new treatments to fight off the novel coronavirus. As vaccines were being developed, scientific research revealed that blood from recovered COVID-19 patients can save the lives of those suffering from severe symptoms.
The COVID-19 virus spreads from tiny droplets released from an infected person’s mouth, and these are smaller than a 1000th of a millimeter in diameter; a droplet around 1mm across can contain as much as 7 million virus particles.

Image: This next-generation microscope enables the observation of living cells at work, capturing cells in attack mode in 3D.
Nowadays, advanced technology has provided powerful microscopes that enable us to visualise the world within our bodies; we can even observe living cells at work and capture immune cells in attack mode in 3D. Other tools such as ultra-high 8K resolution microscopy, 3D reconstructions of electron microscope images, as well as the latest CGI techniques enable us to see the wars between viruses and the cells of our body.
The virus, SARS-CoV-2, belongs to a group of coronaviruses (CoVs) of the Coronaviridae family, namely, the β-CoVs, which infect mammals. Coronaviruses are pleomorphic enveloped particles with a single-stranded RNA genome. There are fringe projections known as spike (S) proteins on the virus’s surface, which are the main characteristic of these viruses. The virus uses the S protein to enter the host cell by interacting with the host cell receptor angiotensin-converting enzyme 2 (ACE2). The viral RNA is released in the host cells and triggers a cascade of events that replicate viral RNA and synthesize structural and non-structural proteins. These proteins are vital in the survival and propagation of the virus.
SARS-CoV-2 is mainly transmitted from human to human via respiratory droplets. When an infected person coughs, sneezes, or talks, another person could be infected if the droplets are inhaled or come into contact with their mucous membranes. The novel coronavirus gets into the body through droplets that carry the virus [e.g. through the mouth, or nose]. However, the virus cannot keep going, and the first barrier it meets is the respiratory tract – the airway that leads into our lungs. The image below shows the repiratory tract magnified more than 10,000 times by an electron microscope.

Image: Human respiratory tract magnified 10,000 times showing tiny hair-like structures called cilia [about a 100th of a strand of human hair] that make tiny rapid movements [over 1000 times per minute]. These movements cause foreign matter such as viruses to be pushed away. However, COVID-19 can infect cilia cells by stopping their sweeping movements in order to slip through and penetrate deep into the lungs.
The novel coronavirus has the potential to infect cilia cells by stopping their protective sweeping movements and slip through into the airways to finally work its way deep into the lungs. When that happens, the COVID-19 infection begins; the virus particules approaches a lung cell and targets an odd looking protrusion on the lung cell’s surface which is only about 1/100000 mm. The novel coronavirus attaches its spike onto that protrusion on the cell surface, then the COVID-19 virus gradually sinks itself into the cell – the infection is now complete! This method is a cunning trick unique to viruses.
Animation: The novel coronavirus attaches its spike to the protrusion on the lung cell’s surface and burries itself into that cell to infect it.
The protrusions [shown in purple in the above animation] which are present on the surface of lung cells, act as a keyhole, only allowing essential substance such as cholesterol. Hence, only substances with the right “key” are allowed to enter the cell. The COVID-19 virus has a fake key that fits perfectly with the keyhole of the cells. So, COVID-19 tricks the lung cell into allowing an intruder inside. The image below was taken with an electron microscope; it shows the interior of a cell that has been infected by COVID-19 [all the red dots are COVID-19 virus particles].
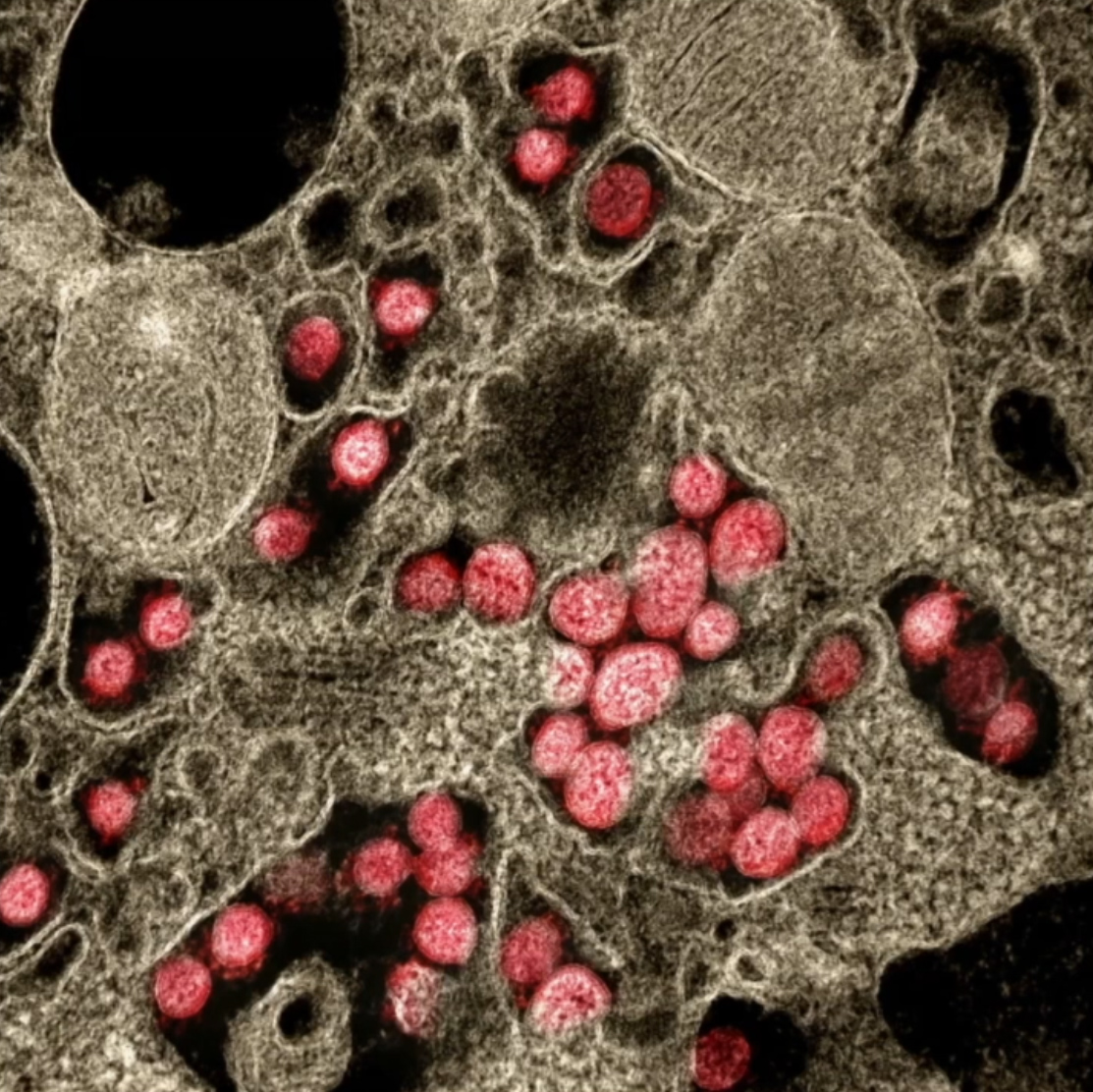
Image: Interior of a cell infected by COVID-19. All red dots are virus particles that once inside can replicate itself as much as a 1000 times before breaking out.

Image: Microscopic image showing the moment where COVID-19 particles [in red] have burst out of an infected cell. Vast amounts of viral particles scatter all around, looking for new cells to infect.
When the COVID-19 burst out and scatter all around from an infected cell while continuing the infection process, patients tend to suffer from more severe pneumonia.
In X-rays of COVID-19 patients, the areas that are inflamed due to the viral infection show up as white spots while the lungs are shown in black; and when the pneumonia intensifies and becomes critical, X-rays show vast amounts of white areas [i.e. vast areas affected by inflammation].

Image: X-ray image of a COVID-19 infected patient. Lungs are shown in black and areas of inflammation caused by the viral infection are shown in white [as these spread, pneumonia symptoms worsen]
In order to prevent such crisis, our body relies on immune cells, which are the defence unit of the human organism. A cell infected with COVID-19 starts to release large amounts of blue particles, a substance called interfera, which sends a warning to immune cells [i.e. our defence units] in order to alert them of a dangerous enemy; this alert [i.e. blue particles] is carried across the body through the bloodstream. Those alert messages are then received by round cells that roam in our blood vessels, known as phagocytes.
Animation: The inside of a blood vessel showing phagocytes on patrol inside these blood vessels all around our body. When they receive the alert message [i.e. blue particles released by infected cells (interferons)] warning them of an enemy intrusion, they head out from the blood vessel to the site of infection
When phagocytes locate their target, i.e. foreign matter such as viruses, they move in and devour it whole, even if those targets happen to be larger than themelves. Patients infected with COVID-19 but who do not show any symptoms are thought to have incredibly active phagocytes in their bodies; those powerful defensive units which engulf the viral enemy are known as our innate immunity and it is part of a system that we have inherited since birth; it derives from our shared evolutionary history of encouters with viruses as human beings.

Animation: Phagocyte devouring the viral target which is larger than itself
But why unlike others, do some people experience life threatening symptoms as their health deteriorates even though they are supposed to be protected by our innate immunity?
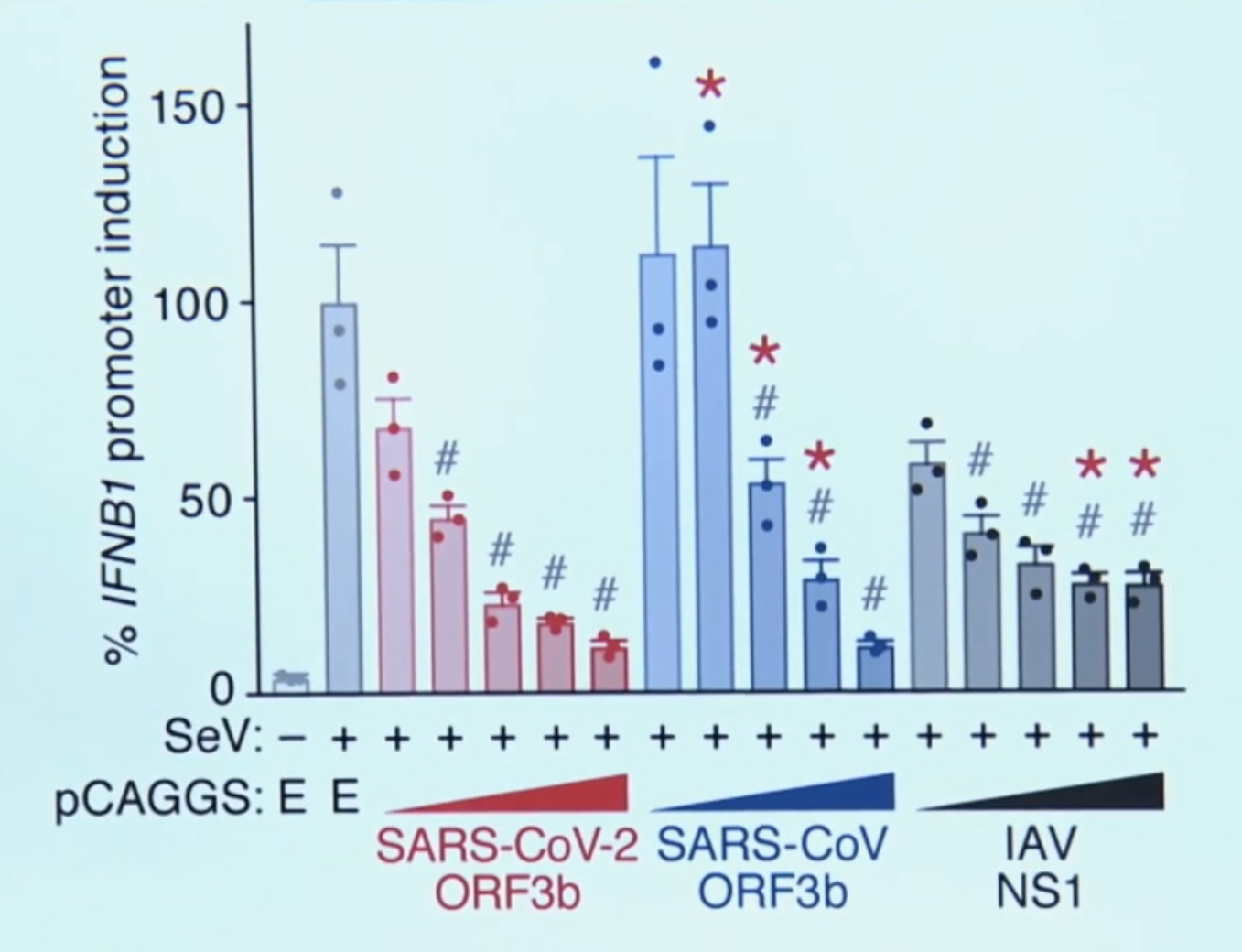
Latest research has revealed an intriguing possibility; the COVID-19 virus may have developed the ability to evade the defensive attacks of our innate immune system. This was uncovered by Dr. Kei Sato at the Tokyo University Medical Research Institute as the genetic information stored inside the COVID-19 virus was explored.

Image: ORF3b, the unique gene of the COVID-19 virus that gives it the ability to deceive the innate immunity of human beings. “The poor IFN responses in COVID-19 patients may be explained by the action of this viral product, ORF3b”, said the lead scientist, Kei Sato
When this genetic information was compared to those of other viruses, the COVID-19 virus was found to have a unique gene [ORF3b, as shown in the image above]. Further experiments revealed that the function of the unique gene discovered was to give the COVID-19 virus the ability to deceive our innate immunity.
Remember, as explained above, a COVID-19 infected cell will release masses of alert messages [i.e. blue particles known as interferons] to warn our immune cells about the presence of a viral enemy. However, when this unique gene [ORF3b] discovered in the COVID-19 virus is activated, those defensive alerts to our immune cells are supressed; only about 1/10 of those warnings are sent [90% blocked] from the infected cell.
Animation: When the unique ORF3b gene that is present in the COVID-19 virus is activated, it drastically reduces the amount of interferons (blue particles) sent by the infected cell [in dark red] to warn the immune cells to take action.
So, when this happens, the phagocytes do not receive any message of the impending danger and hence they cannot be mobilized to neutralise the COVID-19 virus, which is left to replicate itself at will. A further study has found that without the warning messages of the interferons to the phagocytes, the COVID-19 virus can replicate by as many as 10,000 times in only 2 days.

Image: The ability of the COVID-10 virus to replicate and cause severe symptoms is largely related to the patient’s ability to release interferons. Left (with interferons); Right (without interferons); Virus particles replicating itself (in Red)
Now we know that people who experience severe symptoms produce lower levels of interferons, and it is very likely that this weakness in some people allows the novel coronavirus to spread throughout the body and replicate itself savagely, resulting in severe and life-threatening symptoms.
Graph: The number of interferons produced are clearly poor in patients with severe symptoms (Konno et al., 2020)
So, supressing our body’s red alerts is one deadly weapon COVID-19 is using against us and this may be the reason why it has turned into such a global crisis and emergency. Countries around the world and their governments have been stunned by this pandemic and have been taking desperate measures such as complete lockdowns at the cost of their economy in a bid to halt this the spread of this ugly infection.
One of the greatest difficulties with COVID-19 is that there is a certain delay before any convincing symptoms appear and if people are unaware that they are infected, they eventually go on to infect others. Usually, when our body is infected by a virus, an alert substance is released within our bodies, which causes our body temperature to rise in order to activate the immune response. However, since the novel coronavirus is suppressing those warning signals, infected people show no signs such as fever, even thought the viral load within their bodies keeps increasing. That superficially asymptomatic state leads to people not knowing that they are infected and hence allows the virus to spread since those infectious hosts are going unchecked.

Another worrying news is that the virus’s ability to suppress those warning signals seems to be getting stronger with different genetic types of COVID-19 variants spreading throughout the planet. A strain found in Ecuador has a slight alteration in the gene that suppresses the alarm substance. Dr. Paul Cardenas who has been studying patients at the hospital in the capital of Quito said that it is abnormal to find young people developing severe symptoms that quickly. After virus samples of the new strain was collected and analysed, the gene that suppresses alarm signals (i.e. interferons) revealed a mutation; that change leads to the amount of interferons being reduced even further to 1/20. If this powerful variant continues to spread, the immune system’s defence will be forced to fight even tougher battles against the coronavirus.
We have also recently heard a lot about the B.1.1.7 variant [first detected in the UK], the B.1.351 variant [first detected in South Africa] and P.1 variant [detected in Manaus, Brazil]. Other variants continue to appear, such as the one in New York, named B.1.526 which contains the same E484K mutation that has caused so much concern in the UK’s B.1.351 (South Africa) variant; which allows the virus to escape some of the body’s immune response. There are many other variants of COVID-19 appearing around the planet due to genetic changes and these changes will lead to even more variants that could eventually become resistant to the vaccines developed and drugs used to treat patients with severe symptoms.
Vaccines may also have to be updated and modified to address the new variants since those developed for the original virus have been found to be less effective against the B.1.351 (South Africa) variant. The latter variant has been reported to be on the rise in the UK and patients affected by it were on average older and more frequently hospitalised. As for the B.1.526 (New York) variant, it appears to be scattered in the northeast of the US, and its unique set of spike mutations may also pose an antigenic challenge for current interventions. In Finland, The Fin-796H variant, identified by researchers from Vita laboratories and the Institute of Biotechnology at the University of Helsinki, is reported to have mutations similar to those seen in B.1.1.7 (UK) and B.1.351 (South Africa).
The B.1.1.7 variant identified in early October 2020 from genomic sequencing of samples from COVID-19 carriers in the south east of England has been classified as a variant of concern (VOC-202012/1). In December this variant spread from the south east to London and the rest of the UK and its growth coincided with the second national lockdown (5 November to 2 December 2020). Additional control measures had to be imposed after its increased rate of spread with international restrictions on travel from the UK shortly following, in particular to France and to the rest of Europe late in December 2020 to curb the contamination of other countries with this new variant, despite evidence that it had already been present outside the UK. Since then, the prevalence of B.1.1.7 (VOC-202012/01) has been increasing in both Europe and the US. Research conducted in the UK measured the possibility of death within 28 of the 1st positive test result and found that the risk of mortality with the B.1.1.7 (VOC-202012/01) variant is inreased and is high. Hence, as the research carried out by Robert Challen and his colleagues suggest in the British Medical Journal, the UK variant has the potential to raise the mortality rate significantly compared with previously circulating variants, and healthcare capacity planning and national and international control policies are all impacted by this finding as increased mortality lends weight to the argument that further coordinated and stringent measures are justified to reduce human deaths from COVID-19 (Challen et al., 2021).
As of the 30th of March 2021 in France, as predicted by epidemiologists and infectiologists , the UK variant B.1.1.7 identified as “anglais” by the French, has been found to be responsible for the majority of contaminations. Of the COVID-19 positive PCR tests screened to differentiate the original SARS-CoV-2 strain from a variant, 79% of the infections in France were found to be due to the much more contagious “English” mutant B.1.1.7. The share of the South African and Brazilian variants remains is still quite small as the chart below shows.

Pink – UK Variant; Blue – SA Variant; Yellow – Unidentified Variant, and Grey – Original Wuhan Strain / Représentation des variants dans les tests PCR criblés. Source: Geodes, Santé publique France
If the COVID-19 virus manages to evade our innate immune system and keeps on multiplying, in most cases hosts (i.e. humans) remain asymptomatic for around 5 days after they are infected. But when the viral load in the body exceeds a certain limit, symptoms begin to appear in the shape of fever, cough and fatigue. As the virus breaks down our innate immunity and escapes our defences, it continues to replicate at will.
However, the immune system will not just give up. This is when our secondary defence force takes action; it is known as our “Adaptive Immune System” and that is deployed in the fight against the infectious viral invader. This scenario is still dependent on the phagocytes that had been fighting the virus, however now the phagocytes move to a different location and start to act as messengers seeking reinforcements. That messenger phagocyte will attach itself to a blue immune cell while holding a fragment of the novel coronavirus that it had devoured earlier in what looks like a clasp. The blue immune cell will accept this fragment from the clasp and process it as an enemy intel, and will then become activated – it is now a killer T cell ready to attack.

Animation: The messenger phagocyte attaches itself to a blue immune cell while holding a fragment of the novel coronavirus that it had devoured earlier in what looks like a clasp [shown in golden yellow]. The blue immune cell accepts that fragment from the clasp and processes it as an enemy intel, and becomes activated – it is now a killer T cell [shown in green]ready to attack.
These activated killer T cell with information about the virus will now target cells which are infected with the novel coronavirus – it knows what it is looking for. Infected cells have fragments of the COVID-19 virus protruding from its surfaces. The killer T cell will move in and compare those protruding fragments with the information they received from the messenger phagocyte, and if the target matches, it will be confirmed and the killer T cell will will commence their attack; the virus as well as the cell will then be completely obliterated.

Animation: The Killer T cell attaches itself to the surface of the infected cell, compares the fragment in the protruding clasp on the surface with the information it received from the messenger phagocyte and launches its devastating attack once the target is confirmed – obliterating both virus and cell.

Video: We can see the live action from a cutting-edge microscope that has caught the moment of attack by a killer T cell [in green] once it attaches itself to its target cell [in blue]; a toxic substance [in red] is injected, destroying the infected cell along with the alien virus inside.
Unfortunately, it now also appears that the novel coronavirus is finding ways to evade the killer T cell attack. Recent findings from China suggest that the COVID-19 virus has a unique quality setting it apart from other viruses. The novel coronavirus is now targeting those protruding clasps [that hold viral fragments] on the surface of the cells it has infected, reducing their numbers by 60%.

Animation: COVID-19 virus breaking down the clasps protruding from the surface of infected cells, making it much harder for killer T cells to locate them, and allowing the virus to continue multiplying unchecked.
That makes it much harder for the killer T cells to locate infected cells, hence, the infection remains unchecked and the virus continues to multiply in the hosts.
But this war is far from over, since in retaliation our immune system sends out another unit known as the B cells. B cells also get their enemy intel from viral fragments just like killer T cells, however they produce powerful projectile weapons.
Animation: B cells receiving information about the viral target from the phagocyte, and releasing the appropriate antibodies (in Yellow)
B cells release small yellow particles and are shaped as the letter Y when viewed through a microscope; these amazing yellow particles are known as antibodies. These yellow projectile weapons released from B cells close in on the ugly COVID-19 virus and bind to the spikes on its surface [remember these spikes are the fake keys that the virus uses to invade human cells]. Once the virus’s surface is covered with those yellow antibodies, the virus is rendered uselss as it can no longer attach to cells, infect them or replicate. With nowhere to go and hide, they are devoured one by one by the phagocytes. When infected patients reach this stage, they are out of danger, since their bodies will now begin to recover slowly.
Animation: Yellow Y-shaped antibodies produced by the B cells close in on the virus and bind to its spikes. Covered with those amazing antibodies the virus can no longer bind to cells, infect or replicate. With nowhere to go, they are devoured by phagocytes.
Yet, the work of T cells and B cells are far from over, since these amazing defence units will retain their memories of the viral enemy and remain alert in our bodies and ready to fight back for future attacks. These special units study the viral enemy, launch intensive attacks and even after repelling the virus, they will remain vigilant to protect our bodies from harm – it is our adaptive immune system in action.
Vaccines developed against COVID-19 attempt to enhance the power and effectiveness of our adaptive immune system by injecting fragments from an attenuated virus into the body so that information about the novel coronavirus can be passed on safely to T cells and B cells; in that way our adaptive immune system will learn about the enemy before any infection occurs and be ready to provide the necessary attack if infected.
Two studies available as preprints conducted in England found that middle aged women face higher risk of debilitating ongoing symptoms, such as fatigue, breathlessness, muscle pain, anxiety, depression, and “brain fog” after hospital treatment for COVID-19. 7 in 10 patients admitted experiencing “long covid” symptoms an average of 5 months after discharge and those symptoms were more prevalent among women aged 40-60.
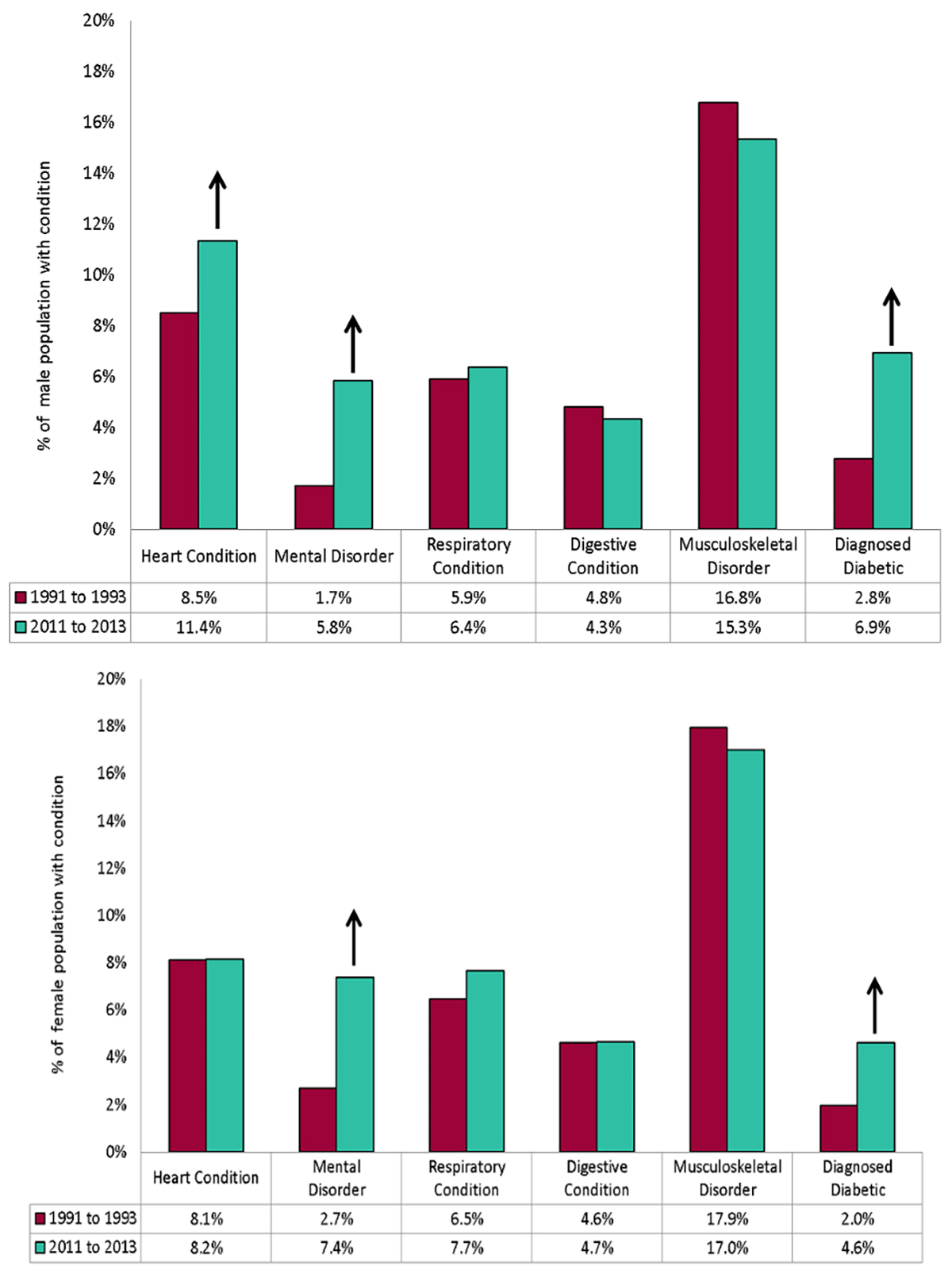
Figure: Prevalence of medical conditions for males & females aged 40 to 60 [Change between 1991 to 1993 and 2011 to 2013 in England / Source: GOV.UK Public Health England
The study carried out in England is reported in the British Medical Journal, it found that among those who classify themselves ethnically as “White”, with 2 or more comorbidities at admission, and receiving invasive ventilation while in hospital the risk was increased; however the severity of acute COVID-19 disease did not affect the likelihood of experiencing long COVID symptoms. [Note: Ethnicity is a grouping of people who identify with each other on the basis of shared attributes that distinguish them from other groups such as a common set of traditions, ancestry, language, history, society, culture, nation, religion, or social treatment within their residing area(s). Ethnicity is sometimes used interchangeably with the term nation]
From the 1077 patients studied, only 29% felt fully recovered when followed up, on average 5 months after discharge. More than 1/4 had clinically significant symtoms of anxiety and depression, 12% had symptoms of post-traumatic stress disorder, 17% had at least mild cognitive impairment, 46% had lower physical performance than age and sex matched controls, and 20% had a new disability. Before being admitted to hospital for treatment, 68% had full time work, but 18% of those had not returned to work and 19% had had to change their working habits due to long-lasting effects. The patients were grouped into 4 clusters by researchers, according to the severity of their physical and mental symptoms post-COVID: Very Severe (17% of patients); Severe (21%); Moderate with Cognitive Impairment (17%) and Mild (46%)
Rachael Evans, a clinical scientist and reseacher from the National Institute of Health Research declared: “The symptoms are very real, but they don’t have a straightforward relationship with heart and lung damage, or certainly heart and lung damage can’t explain all the symptoms.”
A smaller second study, from the International Severe Acute Respiratory and emerging Infections Consortium (ISARIC), found that women under 50 were 5 times less likely to report feeling recovered, 2 times as likely to report worse fatigue, 7 times more likely to become more breathless, and more likely to have greater disability than men of the same age who had been admitted to hospital with COVID-19. Disability usually affected memory, mobility, communication, vision, or hearing. More than half of the 327 patients assessed did not report feeling fully recovered when followed up on average 7 months later, and persistent symptoms were reported by 93.3%, with fatigue and breathlessness the most common.
Chris Brightling, a professor of respiratory medicine at the University of Leicester and a study researcher, speculated that sex based differences in the immune response may be responsible for the higher prevalence of long COVID symptoms in women, noting that autoimmune diseases were more prevalent in women than in men aged 40-60.
“Maybe there’s a difference in the immune response acutely, such that men are more likely to have a more severe condition at the time of the infection,” he told a press conference at the Science Media Centre on 24 March 2021. “It may be that the immune response is different in women, so you then have a continued inflammatory reaction that then leads to a higher likelihood of having long covid.”
Higher levels of C reactive protein, a marker of systemic inflammation were found in patients with the most severe long COVID symptoms. Brightling said that a number of immune and chronic inflammatory condition can also cause elevated C reactive protein. About 450,000 COVID-19 patients have been admitted to hospital in the UK, so a “very large” proportion of these would potentially be affected by long covid, Chris Brightling said, adding, “Clearly there’s an even larger number of people that have had covid in the community, and a portion of those will also have long covid.” (Evans et al., 2021; Sigfrid et al., 2021)

Image: La préparation d’une dose de vaccin. | Photo: Quemener Yves-Marie
Researchers and health departments are working as fast as they can to ensure the safety of treatments and maximise the effectiveness of vaccines. While vaccine campaigns have begun across the planet, many people have lost their lives since the COVID-19 virus appeared in late 2019 and many others are still being infected.
But, what may have happened in the bodies of patients who became critical and ultimately lost their lives?

Image: Casket manufacturing business, South Brooklyn Casket Co. in the U.S, sending a casket to a customer during the COVID-19 pandemic
More than 150 autopsies have been conducted at the University Medical Center Hamburgg-Eppendorf in Germany and something quite unusual was discovered in the lungs of those COVID-19 victims.
Dominic Wichmann: “From our past studies where we learned that with every new disease there are new findings when you do autopsy on a regular basis. We thought it might be very interesting from a scientific point of view to get more into detail in COVID-19. We were really really surprised about very very high incidents of venous thromboembolisms and pulmonary embolisms. We discover that within the first 12 patients, we had about one third of patients who died from pulmonary embolism (Wichmann et al., 2020).”
Pulmonary embolism is a disease where blood clots form in the lungs. Blood clots cause blood circulation to fail in the human body and the resulting lack of oxygen led to the death of those patients. A closer look showed many blue dots among the red clots of blood in those patients; those blue dots are the dead remains of a type of phagocyte called neutrophils that had caused the clots.

Video: Blue dots, which are the dead remains of neutrophils (a type of phagocyte) were found within the blood clots in the lungs of deceased COVID-19 patients
As already explained above clotting occurs when our immune system goes into overdrive, a phenomenon called a cytokine storm. To explain this phenomenon, it is important to understand that the immune cells in our bodies can become overly activated when faced with a virus that is replicating in huge numbers. It has long been suspected that the human body’s own hyperactive immune cells have been damaging the blood vessels, and in order to close those internal wounds, platelets in the blood come would come together to form clots; those grow larger and sometimes end up blocking circulation. The important point to note is that recent research has shed light on this very disturbing mechanism where cytokine storms trigger dangerous blood clot formation.
Yogen Kanthi from the University of Michigan explained: “When Neutrophils start to detect that there are pathogens circulating in the bloodstream, they will start to take their DNA inside of the cell and they expel it outside of the cell. They spit it out from something called a neutrophil extracellular trap (NET). We know that certain cytokines that are released in the setting of COVID-19 can prime the neutrophil and make the neutophil more likely to form NETs (Neutrophil Extracellular Trap).“
What we need to understand is that NETs (Neutrophil Extracellular Traps) are essentially suicide attacks, and this phenomenon was only recently discovered by the academic community in 2004. In normal cases, those kinds of attack will not cause any clotting. But in a cytokine storm overly active phagocytes in our bloodstream self-detonate in excessive numbers – that is where the danger of clotting appears.

Image: The moment of attack: the yellowish-orange phagocyte shown here is only a 100th of a millimeter wide and here it is captured as it self-detonates, hurling its contents (in green) towards the enemy virus (in red). This green weblike structure is the DNA of the phagocyte; the cell sacrifices itself by detonating in a desperate effort to trap the enemy harming the body with its DNA’s sticky texture. (Image courtesy: Max Planck Institute, Germany)

Video: A phagocyte self-detonating and releasing its DNA (in orange), seen here bursting out of that cell. In normal cases, those kinds of protective and self-sacrificing attacks will not cause any clotting. But in a cytokine storm overly active phagocytes in our bloodstream self-detonate in excessive numbers – that is where the dangerous blood clot formation begins
When excessive numbers of DNA NETs (Neutrophil Extracellular Traps) have been cast from the excessive number of phagocytes sacrificing themselves by self-detonating, those can even scatter blood components in the vicinity, lumps from those blood components form clots and bind to each other to grow larger and larger, to the point where they have the potential to completely block blood vessels in the human body. So, despite the intention of the phagocyte to protect its organism, these extreme suicide attacks backfire by forming blood clots that lead to death.

Video: Clots being formed by scattered blood components [formed due to the excessive self-detonations of phagocytes] in the vicinity, binding together and eventually blocking blood vessels
Yogen Kanthi further explains: “COVID-19 as you know, is caused by the SARS-2 coronavirus. And this is a normal virus that our bodies have not encountered before. As a result of that, the bodies don’t know how to respond to it. And so they are pulling out every tool that we have in the toolbox to try and fight this infection. What this means is the infection results in unregulated amounts of inflammation. And so inflammation can be very helpful in the beginning to try and fight off infection and help to repair organs. But if the inflammation is unregulated and continues at high levels for long periods of time that inflammation can be damaging to the body.”
Autopsies carried out on victims of COVID-19 have revealed that blood clots were the direct cause of death for 1/3 of those who lost their lives (Wichmann et al., 2020). Hence, to prevent the formation of deadly blot clots deriving from cytokine storms [i.e. the excessive self-detonations of phagocytes], those cytokine storms must be supressed. This is why drugs to dampen the reactivity of the human immune system have been trialed and considered as potential life-saving treatments in the fight against COVID-19. We are now armed with a new strategy, and hope is on the horizon to help patients with the severest symptoms.
Understanding the Immune System: the legacy of the shared evolutionary history of human primates on planet Earth
In the fight against viruses and pathogens since the dawn of mankind on our tiny blue planet, our immune system has always been the ultimate weapon and its presence can be traced way back in the shared evolutionary history of life. About 550 million years ago, the Cambrian explosion lead to the creation of the wide range of living organisms.

Viruses also existed at that time and are believed to have had spikes on their surfaces; those spikes are the fake keys modern viruses use to infect their hosts. Our evolutionary kin back then looked like a fish, since all life came from water.

Those incredible cells from our adaptive immune system such as T cells and B cells appeared as they endured viral attacks through the course of their evolution with the ability to remember the enemies they encountered and the protective and defensive strategies they used against viruses.
Even if the COVID-19 virus continues to cause panic worldwide, studies have shown that viruses and their hosts have not always been antagonistic towards each other in the course of the evolution of human life on Earth. There are occasions when those viruses and their hosts co-existed, mutually taking advantage of one another. Hence, some viruses are known to have embedded their genes into the DNA of our cells that they had infected. Our early ancestors have also been faced with viruses and were infected by many that permanently left their mark in our DNA; this is a fact of our shared evolutionary history as human primates on planet Earth. As much as 8% of the human genome comes from viruses; and our bodies may have taken advantage of the qualities of those viral genes in its own evolution to gain various important functions.

The process of creating new life itself testifies as a great example. In the process of fertilisation where the sperm binds to an egg, the sperm carrying the father’s DNA has to enter the mother’s egg. Since the egg views the sperm as a foreign substance, the sperm has to use a key to gain entry into the egg. This process is remarkably similar to how a virus enters a cell [as already explained above]. Modern academics and researchers believe that this process comes from the evolutionary past of life on earth; the fertilisation process may have taken advantage of the techniques of viral genes that had infected our early ancestors thousands of years ago.
There are also other functions about humans that are thought to have evolved from viral genes picked up along the way throughout the our shared evolutionary history, such as the placenta, which enables babies inside the womb to receive nutrition and oxygen from the mother, and some brain functions related to long-term memory. Through our long evolution, our immune system became stronger, more efficient and sophisticated.

In the 21st century, we have more than 40 different types of immune cells that are working together in our bodies, forming an elaborate defence network to maintain health and vital functions. While we are eternally evolving along with our cells, viruses too have been evolving, gaining more powerful and elaborate techniques to break through the defences of our bodies. The current war being waged between our immune network and COVID-19 is at its most intense in the shared evolutionary history of mankind. Luckily for us, new insights into the working of our immune system and viruses are providing effective measures to counter the novel coronavirus.
Before the vaccines were released, a patient was infected with COVID-19 and slipped in a coma for 8 days. The first signs were similar to the regular flu, however within 5 days the man had trouble breathing and had to be admitted to hospital and was later transferred to the ICU where he would be put on a ventilator. In these early days against COVID-19, three different drugs were administered to him as part of a clinical trial in a desperate attempt to prevent him from dying, however his condition did not improve – medical professionals were running out of options and time. Then, he was given a special treatment and miraculously regained consciousness within 4 days and a very quick recovery followed. That patient was saved with the blood of another individual who could be said to possess special powers as a COVID-19 survivor. The antibodies contained in the blood of the COVID-19 survivor were collected and injected in the critically ill patient’s body. This treatment is known as convalescent plasma therapy.
Remember! Earlier we explained that: (1) when the virus enters and infects cells, blue interferons are released to alert the phagocytes to take action and devour the viral cells, but since the COVID-19 virus has a mutated gene that supresses the blue interferons, phagocytes cannot be mobilized; (2) the immune system then uses the phagocytes as messenger to carry viral particles as information to the blue immune cell that becomes activated as a killer T cells which then locates protrusions on infected cells’ surfaces to inject toxin and destroy both virus and cell, however, since the virus uses another cunning technique to break down the clasps protruding through infected cells, the T cells fail to detect those infected cells; (3) those 2 solutions were part of our innate immune system, and when they fail the body relies on the adaptive immune system to pass information through phagocytes to the B cells that release the life-saving yellow particles known as antibodies, and when a COVID-19 patient reaches this stage they are out of danger.
That convalescent plasma therapy which saved the above patient’s life is about collecting those amazing Y-shaped yellow particles known as antibodies which are produced by patients who successfully fought the COVID-19 virus. As already explained those yellow antibodies are projectile weapons tailor-made by immune cells based on the information they received on the virus from the messenger phagocytes. We know that antibodies released by B cells engulf the viral cells disabling them and preventing them to replicate, hence these antibodies are powerful weapon that target the COVID-19 virus. Fortunately for the critically ill patient above, the donor’s body was able to produce vast amounts of antibodies from his B cells. When those antibodies were injected in the body of the patient, they successfully disabled and eliminated the virus.
Hence, convalescent plasma therapy treatment is a proven solution expected to save lives as the COVID-19 continues its devastating rampage across the planet. Vaccines may be available, but it will take some time to vaccinate the whole planet, and even if the world is vaccinated, some people may still develop severe symptoms. So, having a stock of convalescent plasma at hand will always be the safest bet in preventing deaths from COVID-19. It seems noble and reasonable for health authorities worldwide to ask COVID-19 survivors to donate their blood, as their antibodies will save lives.

Image: Convalescent Plasma Therapy [Life-saving antibodies created by the B cells of a COVID-19 survivor are collected from his blood, ready to be injected in the body of a patient with severe symptoms]
Research has shown that some individuals have the incredible ability to produce vast amounts of antibodies, enough to save the lives of patients with life-threatening symptoms. Blood was collected from 149 COVID-19 survivors. The graph shows the levels of antibodies found in their blood samples and we can see that they vary from patient to patient; some are able to produce 10 times more antibodies than the average. (Robbiani et al., 2020)

Graph: Level of antibodies produced by the patients who recovered from COVID-19 in the study. (Robbiani et al., 2020)
So what is the difference between people who are able to produce large amounts of antibodies when infected by the novel coronavirus and those who don’t?
The answer to this question is remains a mystery but scientists have a theory. The answer may lie in the moment when antibody production is triggered, i.e. when immune cells holding viral fragments pass on the message [enemy intel] to the B cells of our adaptive immune system which then produce antibodies based on this information. The key here is the shape of the clasp that comes from the messenger immune cell. We know that there are more than 10 000 types of those clasps and they vary from one individual to another.

Image: There are more than 10 000 differently shaped clasps and those vary from one individual to the next
Some clasps have a better grasp [i.e. they can hold on more firmly] to the fragment of the novel coronavirus, hence they keep sending out precise intel to allow large amounts of antibodies to be made. But some people who have differently shaped clasps [i.e. clasps that do not perfectly fit the shape of the viral fragment] lead to their messenger immune cell not being able to grip the viral fragment perfectly, this leads to a lack of precise information being passed on to the B cells, and hence lower amounts of antibodies are released.
Interestingly, we are beginning to understand that these differences may be associated with geography and ethnicity [Note: Ethnicity is a grouping of people who identify with each other on the basis of shared attributes that distinguish them from other groups such as a common set of traditions, ancestry, language, history, society, culture, nation, religion, or social treatment within their residing area(s). Ethnicity is sometimes used interchangeably with the term nation].

People across the planet have inherited differently shaped clasps better suited to fight against the viruses in their area throughout evolution. This evolution is eternal as the human race evolves.
In Africa, for example, we can find many people with clasps that are better suited for holding to fragments of the malaria parasite, meanwhile in south-east Asia there are many people who have the most suitable types of clasps to grip fragments of the bacteria responsible for leprosy. Scientists believe that these differences from different groups from different locations across the planet come from variations in a particular gene known as HLA, which is responsible for shaping the clasps of the immune cells in our bodies.
Katsushi Tokunaga of the Genome Medical Science Project from the National Center for Global Health and Medicine explains: “Many types of pathogens have emerged throughout our history. In different regions at different ages. That is why mankind has acquired different HLA types to fight off different pathogens.”
About 200,000 years ago, our ancestors, the early primates, left Africa and began to explore and migrate to different parts of the planet. Wherever they moved to, just like us today, they also had to face viruses and pathogens. After each attack, it is believed that their immune system and HLA gene adapted; so these clasps suitable to face new enemies have been passed on to us through the long journey of evolution.

Image: Each individudual has inherited a uniquely shaped clasp from their individual evolutionary history
Katsushi Tokunaga: “The diversity of HLA’s is our defense against the range pathogens. So only those who excelled in the fight against them left their HLA types as a legacy to us.”
We still cannot know when or how some individuals have acquired the incredible ability to develop those amazing clasps that are so well adapted to fight off the COVID-19 virus; the most rational explanation seems to be that individuals in their evolutionary lineage in the past experienced infections from viruses that shared a great deal of structural similarity with the novel coronavirus, hence they have acquired clasps that just happen to perfectly fit the shape of the COVID-19 virus. Every individual on our planet has inherited different shapes of clasps within their immune cells to fight off viruses. This is our heritage from our shared evolutionary history as primates on earth and a testament to our primitive ancestors who had fought and survived an incredible variety of infections diseases throughout evolution.
Today, cutting-edge medicine is attempting to harness the immune super powers of the few incredible individuals so that lives all over the world can be saved by passing down their immunity [i.e. the antibodies created by their B cells ]to fellow humans.
At the Lilly Technology Center, scientists are culturing immune cells collected from those individuals with super powers who can produce large amounts of COVID-19 antibodies. They are hoping to produce antibodies in vast quantities so they can be used to save the lives of patients suffering from the severe life-threatening symptoms of COVID-19 worldwide. Clinical studies are already underway and the academic community is hopeful that convalescent therapy treatment will be widely available.
Pamela J. Bjorkman from the California Institute of Technology Eppendorf said: “I think we could make things in the laboratory that would work better than what people are making. And maybe those would work at very low concentrations and make a practical way of delivering to people to protect them or help them if they’re actually sick. This is definitely a possibility. And I think it’s a very hopeful one too. If anyone was sick and they were willing to donate their plasma to help other people and to help science, then yes, they are definitely heroes.”
The planetary war agains COVID-19 continues with no end in sight. However, it is important to note that our immune networks have been supporting us since birth and will do so until we take our last breath.

From birth, the moment we leave the vagina and take our first gasp of air on this planet as infants we are exposed to many different pathogens like viruses and bacteria. But the immune cells of babies are not yet ready to fight back. The first protection for the baby comes from the mother’s breast milk, which contains large amounts of immune cells and antibodies belonging to the mother; those help the baby’s own immune cells to develop while also providing protection from various bacteria and viruses.
Image: Des mères allaitant leur bébés / Mothers breasfeeding their babies
After several months, the baby’s own immune networks begin to kick in, and in the years that follow through exposure to various types of viruses and bacteria our immune system continues to develop and grow stronger. It had previously been thought that the immunity of human beings reaches its peak around 20 years of age and then flattens out, gradually declining at around the age of 70.

But during the current COVID-19 pandemic incredible recoveries have been observed across the planet from individuals in the 70s, 80s and even some centenarians. Studies suggest that these incredible individuals have something “special” in their bodies that is keeping their immune cells young.

3 COVID-19 survivors who are above 90 years of age: (i) Connie Titchen (106, from the UK); (ii) Albert Chambers (100, from the UK); and Maria Branyas (113, from Spain)
The mystery of the human body remains and we know that it is a remarkable system supported by specialist cells that protect our lives with their unique skills honed over 4 billion years of evolution. The keys to overcoming this pandemic and future ones might just be locked away in our own bodies and it could be hidden in some incredible individuals out there.
It is important to note that these findings are just the beginning, and it will take years of serious research to fully understand COVID-19 along with the range of cardiovascular and immune effects it might trigger as new variants continue to evolve. We can only hope to find a way to stop this ugly virus in its track through the combined efforts of planet Earth’s scientific force and medical geniuses.
At present, whilst COVID-19 appears to be more contagious than SARS or MERS, the fatality rate is relatively low (around 3%) when compared with MERS (34%) and SARS (10%), with early data suggesting the elderly and those with underlying health conditions are at a higher risk.
In France, if Mentonians are concerned about coronavirus, it is in fact mainly for their elders. « Menton is a town of old people. If the epidemic spreads, they’ll all be dropping like flies. It’s going to be no man’s land, » said Denis, arm in arm with his 88-year-old mother. « I’m not afraid for myself: I know the virus won’t kill me. But I’ve told my mother, ‘you’re not going out of the house any more,’ » explained Véronique, in her fifties, as she folded a tablecloth from her shop in the centre of town.
By advocating the use of chloroquine to treat people suffering from Covid-19, the brave maverick, Professor Didier Raoult became the target of criticism in a very short time. Raoult did, however, receive some support, notably from Jean-Marie Bigard, who recounted one of his telephone conversations with the much-scorned professor. « We talked about how he thanked me for supporting him (…) And then he said something funny to me, saying: ‘All the time I was thinking about this story, I only thought about one thing, and that was your sketch about the bat,’ » the comedian said. Furthermore, even if it is not a miracle cure, a range of other medical professionals claim to have successfully treated a range of COVID-19 sufferers with hydroxychloroquine, while some studies have shown its ability to inhibit the virus in vitro.

Image: Didier Raoult au micro d’Apolline de Malherbe
Didier Sicard a professor from Sorbonne University also a specialist in infectious diseases who has a long experience in scientific work on the HIV, argued that researchers should go back on the field and inquire on the animal origin of the epidemic. Professor Sicard noted that the abrupt transformation of primary forests has brought humans closer to bats and hence a reservoir of viruses that has not yet been closely studied.
While China has only recently, on the 24th of February 2020, immediately and completely banned all traffic and consumption of wild animals, conscious of its dietary culture of eating practically anything that moves, it is important to note that such a legislation exists since 2003 without it being strictly respected by Beijing. Hence, Professor Sicard reasonably argues for an international health court. The former Chair of the Advisory Committee on Ethics from 1999 to 2008 emphasizes the extent to which, in this epidemic, the issue of contact is paramount – everyone must behave like a model.

Image: Femme consultant son médecin / Woman consulting her doctor Source: AFP – B. BOISSONNET
Sicard also points out that the starting point of this pandemic is an open market in Wuhan where wild animals, snakes, bats, pangolins, preserved in wicker crates, accumulate. In China, these animals are bought for the Rat Festival and are quite expensive and considered as food of choice. In this wild meat market, these animals are obviously touched and handled by the vendors throughout the day, skinned, while they are stained with urine; ticks and mosquitoes also make a kind of cloud around these poor animals by the thousands.
These conditions have meant that a few infected animals have inevitably infected other animals within a few days. One can hypothesize that a vendor injured himself or touched contaminated urine before putting his hand to his face. Here we go! What strikes Sicard is the indifference at the starting point of this ugly virus. As if society was only interested in the point of arrival: the vaccine, the treatments, the resuscitation. But for this not to happen again, the starting point should be considered vital. And it’s impressive to see how it’s being neglected. The indifference to wildlife markets around the world is dramatic. It is said that these markets bring in as much money as the drug market. In Mexico, there is such a traffic that customs officers even find pangolins in suitcases.

Image: Un pangolin sauvé au Mexique par la Wildlife Alliance / A pangolin being rescued in Mexico by the Wildlife Alliance

Chart: Estimated number of Asian pangolins in international trade between 1977 and 2012 as reported to CITES, and estimated number of pangolins in illegal trade in Asia between July 2000 and 2013. Illegal trade is based on seizures made in or trade recorded in Cambodia, China, Hong Kong SAR, India, Indonesia, Lao PDR, Malaysia, Myanmar, Nepal, Pakistan, Philippines, Singapore, Sri Lanka, Taiwan (P.R. China), Thailand and Vietnam. Source: CITES trade database (UNEP World Conservation Monitoring Centre, Cambridge, UK), and for illegal trade, various sources / Source: (Challender, Harrop and MacMillan, 2015)
Jean-Christophe Ruffin, a doctor, diplomat and writer from the Académie Française said: “Now is not the time to burden anyone and sue, it will come. But they’ll have to be done. We’ll have to learn from this. This proves one thing: when we get out of this terrible crisis, as infectious disease specialists say, there will be others. And we can’t be in a situation like that again.”
« It is of course not the first time that animals are at the origin of sanitary crises, in fact they are responsible for the majority of epidemic crises: HIV, H5N1 avian flu, Ebola. These viral diseases always come from a reservoir of animal viruses », Sicard pointed out, and there’s almost no interest in them. It’s the same with dengue fever. “I have a very close relationship with Laos, and when the disease appears, the local people there say, ‘We have to control the mosquitoes’. But in reality, it is during the dry season, when there are only larvae, that a policy of exterminating mosquito larvae should be implemented. But nobody does it because people say ‘oh, there are no mosquitoes, why do you want us to use insecticides? And the Pasteur Institute of Laos is sputtering in vain, asking local people to make the effort before the disease bursts”, Sicard explained to France Culture, saying “It is exactly like the work that’s left to be done on the bats. They are themselves carriers of about 30 coronaviruses! We need to do some work on these animals. »

Image: Pangolin sauvé des mains d’un trafiquant local, Uganda. 9 avril 2020 • Crédits : Isaak Kasamani – AFP
The latter also added: « Obviously, it is not very easy: going into caves, well protected, taking vipers, pangolins, ants, looking at the viruses they harbour, this is ungrateful work and often despised by laboratories. Researchers say: ‘We prefer to work in the molecular biology laboratory with our cosmonaut hoods. Going into the jungle, bringing in mosquitoes, is dangerous. Yet, these are by far the most important routes.
Moreover, we know that these epidemics will start again in the years to come repeatedly if we don’t definitively ban the traffic of wild animals. This should be criminalized as an open-air sale of cocaine. This crime should be punishable by imprisonment. I am also thinking of those battery farms for chicken or pork that are found in China. Every year they give new flu outbreaks from viruses of avian origin. Gathering animals like that is not serious. It is as if veterinary art and human medical art had nothing to do with each other. The origin of the epidemic should be the subject of a major international mobilisation.”
Prof Sicard argued that we need to reconstruct the epidemiological pathway by which bats have tolerated coronaviruses for millions of years, but have also dispersed them. It contaminates other animals.

Letko, M., Miazgowicz, K., McMinn, R., Seifert, S., Sola, I., Enjuanes, L., Carmody, A., van Doremalen, N. and Munster, V., 2018. Adaptive Evolution of MERS-CoV to Species Variation in DPP4. Cell Reports, 24(7), pp.1730-1737.
When bats hang in caves and die, they fall to the ground. Then the snakes, vipers in particular, who love their corpses, eat them. Just like the young bats that fall down and are immediately eaten by these snakes which are therefore probably intermediate hosts for viruses. In addition, there are clouds of mosquitoes and ticks in these caves and we should try to see which insects are also possible transmitters of the virus. Another hypothesis concerns the transmission that occurs when bats go out at night to eat fruit. Bats have an almost automatic reflex; as soon as they swallow, they urinate, explained Sicard. They will therefore contaminate the fruits of these trees and the civets, which love the same fruits, hence contaminating themselves by eating them. The ants participate in the agape and the pangolins – for which the most wonderful food is ants – devour the ants and become infected in their turn. It is this whole chain of contamination that needs to be explored. Probably the most dangerous reservoirs of viruses are snakes, because they are the ones that are constantly feeding on bats, which are themselves carriers of coronaviruses. Snakes could therefore be a permanent host for these viruses, and obviously eating them is not only disgusting but dangerous. But that is exactly what we need to know and check. Researchers should therefore capture bats, but also do the same work on ants, civets, pangolins and try to understand their tolerance to the virus. It’s a bit ungrateful, but essential.
Didier Sicard also elaborated on the relation between the local Eastern Asian population and the bats, saying “What struck me in Laos, where I often go, is that the primary forest is regressing because the Chinese are building stations and trains there. These trains, which cross the jungle without any health precautions, can become the vector of parasitic or viral diseases and carry them through China, Laos, Thailand, Malaysia and even Singapore. The Silk Road, which the Chinese are in the process of completing, may also become the route for the spread of serious diseases. Caves are becoming more and more accessible there. As a result, humans tend to get closer to where the bats live, and bats are also a highly sought-after food source. Humans are now also building fruit tree parks close to these caves because there are no more trees due to deforestation. The inhabitants feel that they can gain territory, like in the Amazon. And so, they are building agricultural areas very close to extremely dangerous virus reservoir areas. I don’t have the answer to all these questions, but I just know that the starting point is not well known. And that it’s totally ignored. It’s being turned into folksy conference speeches. They talk about bats and the curse of the pharaohs.”
Sicard also said that there must be some serious studies about the ability of bats to harbour coronaviruses, saying “but when I go to the Pasteur Institute in Laos which is run by an exceptional man, Paul Brey, this director has the fibre of a Louis Pasteur, he has been passionate for twenty years about transmission issues, but he is extremely lonely. Even the study of mosquitoes, which is fundamental to understanding the transmission of diseases in Laos, is almost abandoned. And Paul Brey keeps telling me that there are about thirty species of coronavirus in bats. So, the scientific effort is not up to the task.” Sicard added, “When the French Ministry of Foreign Affairs removes the virologist’s post at the Pasteur Institute, which is a few hundred kilometres from the Chinese border, we are finished. This happened in November 2019. We are going to try to get that post back, but it is still frightening to think that even at the very gates where viral infectious diseases come from, it is hard to put all the effort into it. The Pasteur Institute of Laos is supported very moderately by France, it is supported by the Japanese, the Americans and the Luxembourgers. France contributes to it, but it does not make it a major research tool.”
The role of this Pasteur Institute according to Professor Sicard is to train local researchers, “To carry out epidemiological studies on the existing viruses chikungunya, dengue fever and now coronavirus, to be a place for high-level biological scientific studies in a remote, tropical territory, but with a high-security laboratory. To be as close as possible to where epidemics occur and to have laboratories that are up to the task. It is very difficult for relatively poor countries to have high level scientific equipment. The network of Pasteur Institutes – which exist in several countries – is a structure that the world envies. But institutes like the one in Laos need much more help than they do now. These laboratories are struggling to make ends meet and they are also having difficulty recruiting researchers. Most of them prefer to be in their laboratory at the Pasteur Institute in Paris or in a Sanofi laboratory or at Merieux, but to become an explorer in the jungle, there aren’t many people who do that. But that’s what Louis Pasteur did, he went to see the farmers in the vineyards, he went to see the shepherds and their sheep.»
Traduction(EN): « Science has no homeland, because knowledge is the heritage of humanity, the torch that lights up the world. » – Louis Pasteur
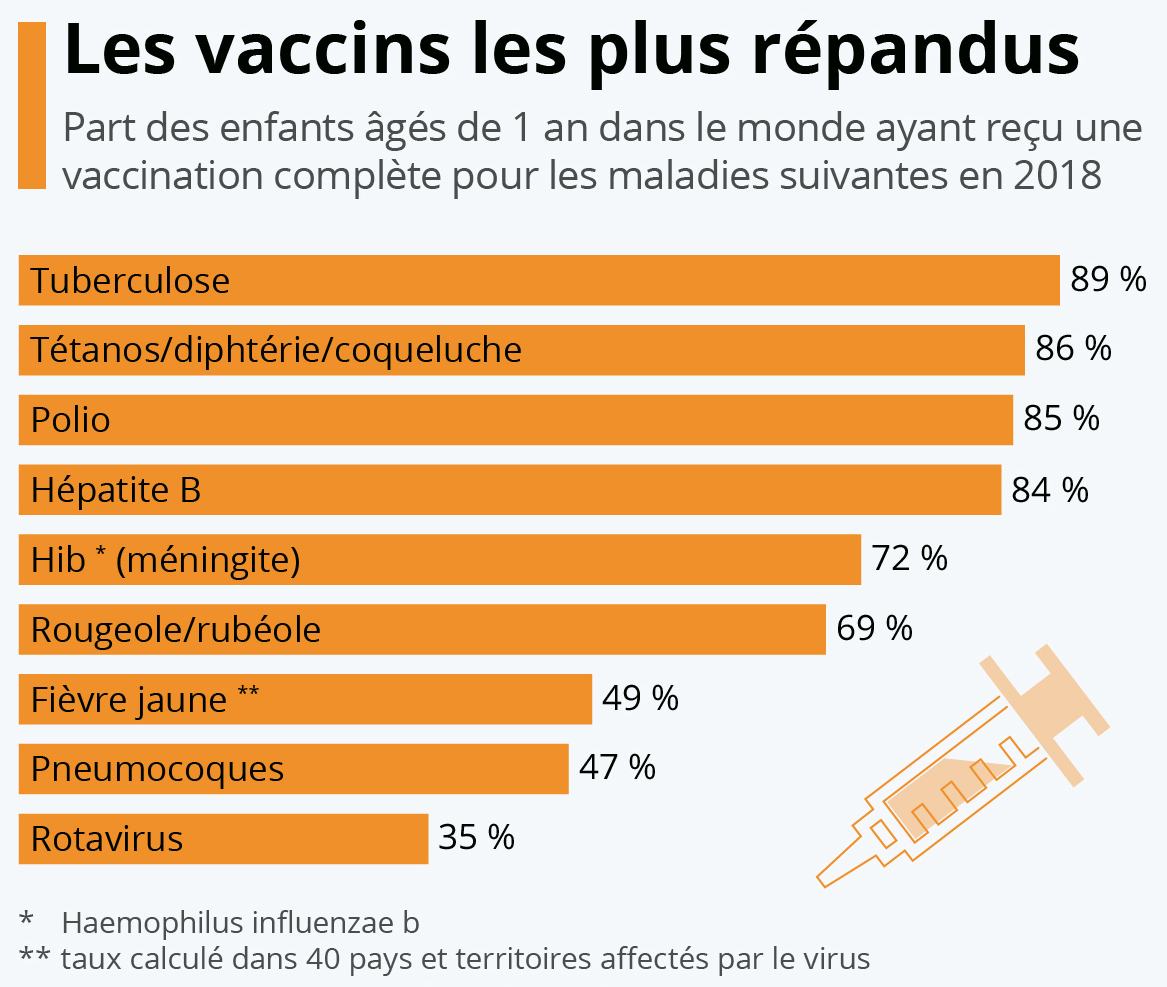
Les vaccins les plus répandus / The most common vaccines (Source: Statista France)
Science is an integral part of human culture and has played a huge part in the construction of the modern societies that humanity lives in today, and I believe the essay, “History on Western Philosophy, Religious cultures, Science, Medicine & Secularisation” gives a decent picture of where we came, where we have come and where we are going as a civilisation. « Louis Pasteur would come out of his laboratory. Just like Alexandre Yersin who was in the field in Vietnam when he discovered the plague bacillus », Sicard declared, « so, entomological research and research on transmitting animals is not up to the challenge. Of course, it exists, but it must account for perhaps 1% of research. Because what fascinates the candidates for the Nobel Prize is to find a treatment or a new virus in molecular biology and not to reconstitute the epidemiological chains. And yet the great infectious discoveries were born this way: the agent of malaria, Plasmodium, was discovered by a Frenchman, Alphonse Laveran, in the field in Tunisia. And this is fundamental research that is carried out on a scale that has been somewhat forgotten. »
Is the study of animal really crucial? Sicard said: “The plague remains an exciting example. The reservoir of the plague are rats. There are populations of rats that are very resistant and that transmit the plague bacillus, but they don’t care. And then there are populations of rats that are very susceptible. All it takes is a few individuals from the susceptible rat population meeting the resistant rat population one day to get infected. The susceptible rats die. At that point, the fleas that feed on the blood of the rats, desperate not to have more live rats, will start biting humans. Reconstructing this very beginning of the chain of transmission makes it possible to act.
In places where the plague is still rife, in California, Madagascar, Iran or China, when we see that a few rats start to die, that is exactly the time to intervene: it is extremely dangerous because that is when the fleas will start to want to bite humans. In plague areas, when we see hundreds of dead rats, it is a real bomb.

Tableau: Le Triomphe de la Mort, par Pieter Brueghel l’Ancien, 1562 (Huile sur bois). Ce tableau est une allégorie mettant en scène diverses formes relatives à la mort : crime, exécution, maladie, combat, suicide.
Fortunately, the plague is a disease of the past. There must still be 4,000 or 5,000 cases of plague in the world. That is not a huge number and then the antibiotics are effective. But this is an example, to show that the animal origin is fundamental and always difficult to apprehend. It is nevertheless essential for understanding and makes it possible to put in place prevention policies. Today, if we continue to sell wild animals on a market, we are in a delirious situation. The precautionary principle must be applied.”
While wild animal traffic is prohibited and there is an international convention that monitors all sales, in China this international convention is not respected, declared Sicard, adding “It is clear that if we ask each country to organise itself nationally, nothing will change. China initially put pressure on the WHO not to call it a pandemic. It tried to block it because it is a major contributor to the funding of the WHO.
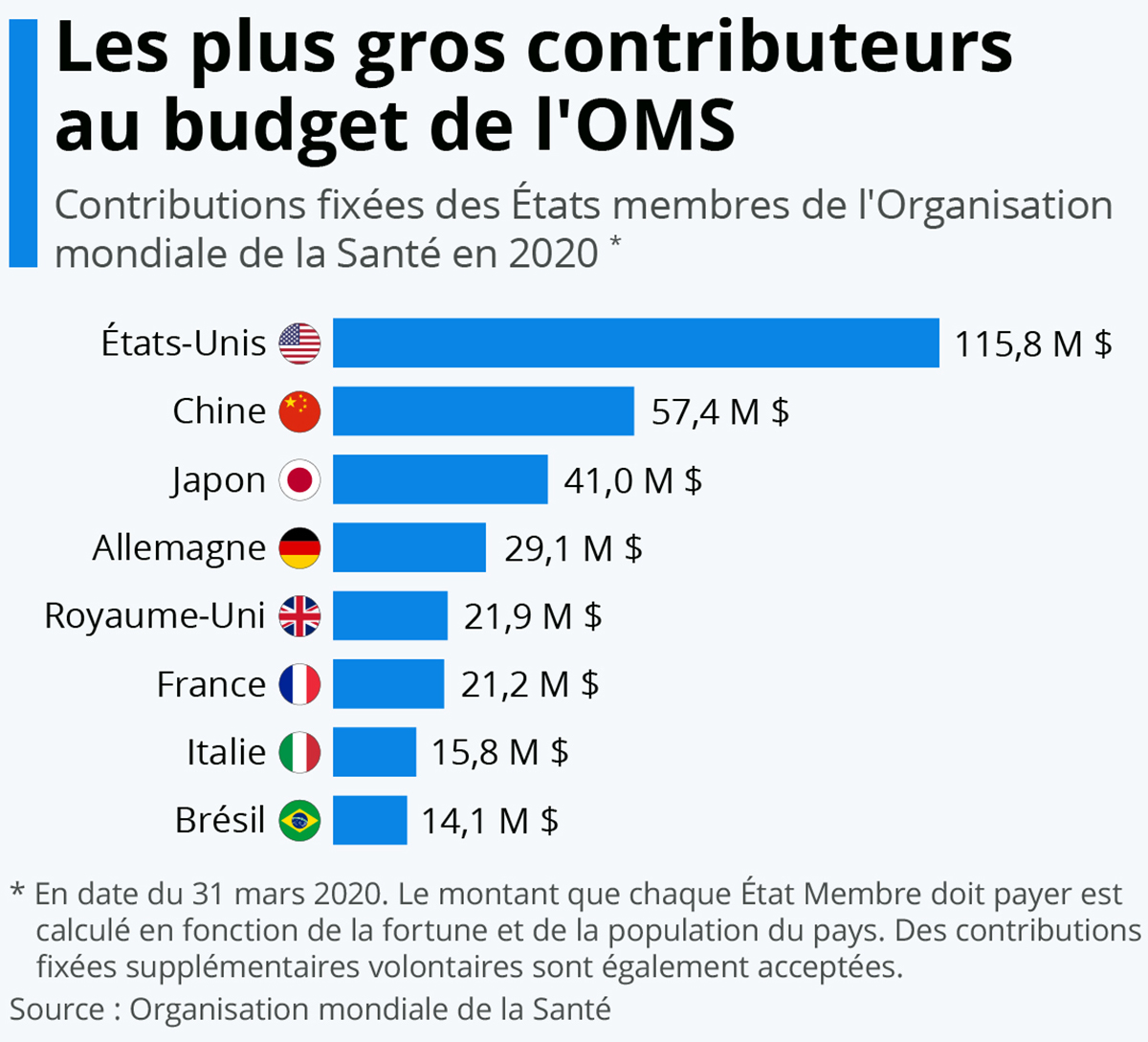
Les plus gros contributeurs au budget de l’OMS / Source: Statista France
It would therefore be important for it to be a totally independent health tribunal, like an international war crimes tribunal, with independent inspectors who verify what is happening on the ground. In Laos, in the countryside, there are many markets where wild animals are sold like chickens or rabbits. There is general indifference because it is the local culture. And culture is the most difficult thing to change in a country,” observed Didier Sicard. Indeed, rightly concluded, since culture, which is a mode of behaviour passed down by individual groups to other generations unfortunately is also sometimes constitutive of a range of atrociously bad and unproductive habits [e.g. medical, dietary, physical (health), linguistic, educational, artistic, perceptive, emotional, managerial and political patterns].
« Avant, avec mes amis, on avait peur des Chinois. Maintenant, on voit sur Twitter qu’on a peur de nous, les Italiens ! »
Alicia à franceinfo
Sicard also commented on what struck him on the attitude of the French population, stating, “the gap between a kind of indifferent casualness, hardly any critical look at Italy and China and the brutal discovery of the health disaster. We have gone from recklessness to extreme anxiety and both are equally toxic: recklessness creates contamination and extreme anxiety leads to irrational behaviour. The proof of this is the flight of Parisians, Lyonnais and inhabitants of large cities to their second homes. This seemed to me at first to testify to a very short-sighted vision, as if one could escape, in war, from the arrival of the German armies. And then an extraordinarily individualistic behaviour, in the wrong sense of the word: ‘Save whoever you can, I shut myself up in my countryside and then it’s too bad for the others, I protect myself’. Of course, I imagine that if you can protect the elderly and keep them safe, that’s fine. But when we see young couples or groups of friends who are now saying to each other, we’re going to go on holiday! This is all the more shocking because this epidemic is about something completely different from just saving someone. On the contrary, it’s a question of asking how each can be seen by the other as a role model.”
Professor Didier Raoult also pointed out in 2009, that human civilization is still savage and prehistoric when it comes to a culture of medical hygiene because most of us do not know how to handle viruses due a lack of knowledge and social organisation, i.e. it is a pattern of behaviour that is still not firmly embedded in culture of the non-scientific majority. Raoult even pointed out 11 years ago that if a mutant respiratory virus was to appear we would be facing a considerable disaster, and here we are.
Didier Raoult « On ne sait pas lutter contre la contagion d’un virus respiratoire » | Archive INA (2009)
A similar argument was also recently brought forward by Bill Gates in 2018 who suggested that a new diseases could kill 30 millions in 6 months, while his foundation published a simulation showing an epidemic spreading from China, which is coincidentally now facing a « serious situation » to deal with the accelerating deadly coronavirus epidemic that has put the world on its knees. « In the case of biological threats, that sense of urgency is lacking, » Gates said, adding that countries need to prepare for pandemics in the same serious way they prepare for war; he asserted that a small non-state actor even had the ability to construct a deadly form of smallpox in a laboratory environment. The philanthropist explained in an interview on Virtual TED Interview that if the United States enacts such a strict isolation law, positive results could be seen within the first 20 days. According to Gates, the United States was too late to react. If they had started testing people who might have had the virus as early as February, they could have escaped total isolation. « There are no half measures. It’s not right to say « keep going to restaurants and buying houses, ignore the pile of dead bodies in the corner. It’s irresponsible to tell people not to worry, » said Bill Gates, also adding that the public must, at all costs, maintain the law of isolation for as long as it is necessary to save lives and prevent the situation from becoming similar to that in Wuhan and Northern Italy.

#COVID19 : en se basant sur des modèles prédictifs, des chercheurs de l’UCL ont estimé que l’ensemble des mesures de #confinement ont déjà permis de sauver plusieurs dizaines de milliers de vies en Europe / Source: Statista France
In an essay written on the Oxford Martin School website at the University of Oxford Ian Goldin and co-authored by Robert Muggah, a similar orientation is suggested, i.e. for the world to become more interdependent since our world has become more connected. However, globalisation must be managed efficiently in order to fight systemic risks such as the COVID-19.
We saw how the growing complexities of the global financial system was badly managed by public authorities controlled by politicians, and supposedly financial « experts », people who were supposed to have graduated from the supposed best institutions, simple parvenus turned mechanical thinkers, and what did they do? Together, as a pack of ruthless & cannibalistic great white sharks, they took the whole world into the financial crash in 2008; it is not even the first time in history and nothing tells us that they will not do it again. The full blame can be attributed to the dangerous negligence and overconfidence of this very special and particular breed.

Image: Un banquier assis dans la rue / A banker sitting on the street
This has led to mediocre, cheap, uncharismatic and atavistic populists politicians without any sophisticated outlook about a connected world to storm to power since the world’s political and economic « elites » were held responsible for the 2008 financial crisis. But we now see how these populists lack the sophistication to lead a new modern and interconnected world as we are living through this crucial phase in human history where civilisation is changing era with the post-modern technological revolution [The sincere, realist, punching, unhypocritical, genre-defying, barrier-smashing, universal and mind-blowing documentary by fellow Frenchman Nicolas Hulot about the impact of humans on environmental change released in 2009, « Le Syndrome du Titanic » portrays this change of era magnificiently – unfortunately those types of production seem far too honest, scary, deep, profound and intellectually stimulating to get the publicity and attention they deserve among the mainstream consumers and the industries who have everything to gain in them remaning naive and atavistic, but remains an iconic piece in the collection of the wise, avant-garde & insightful chosen few – facts that can never be hidden]
The atavistic minds who grabbed power in the US are following an ancient tradition that does not have its place anymore in our modern world, i.e. blaming foreigners for everything and turning their back to the outside world, and hence also making themselves insignificant among noble world leading societies, i.e. those who together set an example to civilisation and shape the human civilisation of the future.

Une majorité de 80% des citoyens français se méfient des Etats-Unis et n’approuvent pas leur politique / Source: Le Figaro
The grotesque US president, Donald Trump spurned scientific thinking about a range of serious issues such as climate change, spread fake news through petty news agencies and twitter ogres and even shunned traditional allies and international institutions such as the World Health Organization and the Paris Climate Agreement, decisions that have not been met with approval by many sensible Americans; for example, Melinda Gates sees Trump’s decision as absurd, and with the evidence of infections rising fast, most extremist nationalist politicians are compelled to recognise the traumatic human and economic costs of COVID-19. Hence, it is also not surprising that in France, a literary, intellectually hungry and constantly evolving nation of voracious and sophisticated self & world-cultivating book readers & writers, Trump is viewed as one of the greatest disasters of the modern world, compared to the pigs of George Orwell’s « Animal Farm », and has even been paraded as a clown along with Macron in Nice.

« Complice du pire » / Trump le clown et Macron la marionnette au carnaval de Nice, 2019 / Source: 20minutes
« Do me a favor, speed it up, speed it up. », this is what the naive Trump told the National Association of Counties Legislative Conference, because the ignorant, infantile, insensitive and obese politician believed that if he repeated it a couple of times the vaccine would have suddenly appeared. A vaccine takes longer to be safe and ready, and most people with some scientific foundation know this. As the American chemist, inventor, musician, professor, entrepreneur and former chancellor of the University of North Carolina, Herbert Holden Thorp wrote for ScienceMag, China has rightfully taken criticism for blocking attempts by scientists to report the truth about the coronavirus, the US under Trump and his circus have been doing the same thing. To inform Fauci and other government scientists that all public comments must be cleared with Pence is bordering on dictatorship and an assault on individual freedom and dignity.
It is clearly not a time for a mediocre, disconnected, unsophisticated and atavistic American politician who does not fear ridicule by making an absolute ass of himself through his denial of evolution, climate change and the dangers of cigarette smoking to come around and tell people how to live, what to believe in and shape the public message; this is dangerous to every single person who lives in the US. It is however encouraging to see that Fauci, Francis Collins [director of the U.S. National Insitutes of Health (NIH)], and their colleagues across federal agencies ignored these instructions and gradually spread the message, because transmission rates and death are not measurements that can be changed with Trump’s will and an extroverted presentation. The Trump administration repeatedly lied, saying that the virus spread in the US was contained, when it was very clear from genomic evidence that community spread was occurring in Washington State and beyond. This kind of distortion during such a deadly pandemic is unacceptable and contributed to the federal government’s slow response. Although the words of the Trump administration have never mattered to or registered in the brain of learned individuals, these words are now clearly a matter of life and death in the US during the pandemic.
Most intellectually cultivated, smart and refined individuals do not expect politicians or mediocre gossip journalists to know much about philosophical discourse, the foundations of scientific reasoning, objectivity, statistics, to be able to read and fully understand a scientific paper, let alone understand brain physiology, the laws of evolution and gravity, p-value, logical reasoning or know what ostinato and legato are; and that is perhaps why most of the finest intellectuals remain in their league and keep their distance from street politicians and the common crowd, because they likely know that it would be like trying to communicate with non-receptive, indifferent and inanimate objects such as pebbles or truffles.

Image: Truffes blanches / White truffles
Hence, it is very likely that to most sensible and intellectually cultivated individuals, attempting to have a conversation with those objects would be a waste of time, neuronal activity and calorie; while also having to leave the noble realm of philosophical discourse, their library with names such as Darwin, Voltaire, Balzac, Descartes, Rousseau, Lacan, Satie and Debussy, and sometimes even their piano or violin, to then have to jump into a world of slimy reptilian characters and see weird and untrustworthy faces of brains inferior to their own trying to tell them how to live, and also having to endure mockery of the lowest, most infantile and animalistic kind from some of the vilest and most frustrated peasant-like parvenus in politics with severe inferiority complexes. So these cultured intellectuals keep quiet in the distance and focus on writing books instead.

Source: Services culturels – Ambassade de France aux États-Unis / Cultural Services – French Embassy in the US
As a bilingual Franco-British intellectual, in the French speaking world for me, it would be like attempting to have a sophisticated discussion about « les métaphores artistiques d’Eugène Delacroix, la structure du psychisme, la philosophie du désir, la motivation chez le sujet cartésien, l’héritage voltairien, et la dialectique Lacanienne » with « simplets » [i.e. simple minds] like Bécassine, Nabilla, Bamboula, Darmanin, Hollande, Pompili and Morano in a small village bistrot; and in the Anglo-Saxon sphere with Postman Pat, Nigel Farage, Harry Potter or Mr.Bean in an ancient and derelict pub in England, or Homer Simpson, Forest Gump, Joe Biden and Donald Trump in the US – so, what I mean and what most intellectually superior individuals understand is that it would be useless and unproductive because of the unsynchronised psyches caused by different levels of intellectual cultivation and heritage.
If the majority of humans read, manage to grasp and fully understand the essay, « Psychoanalysis: History, Foundations, Legacy, Impact & Evolution », they should realise that the human psyche, its development, cultivation and construction are composed of many layers, while the essay, « The Concept of Self » would also guide individuals about self-conception and identity. After studying intellectual humility, psychologists have found that individuals with this personality trait have superior general knowledge (Krumrei-Mancuso, Haggard, LaBouff and Rowatt, 2019). Intellectual humility has consequences for learning and styles of thinking; the process of learning itself requires intellectual humility to acknowledge that one lacks a particular knowledge and hence has something to learn in order to continue evolving. In the same study in the Journal of Positive Psychology, Krumrei-Mancuso and her colleagues found that intellectual humility was associated with less claiming of knowledge that one does not have, indicating a more accurate assessment of one’s own knowledge. In the study, intellectual humility was also correlated with being more inclined to reflective thinking, and also possessing more “need for cognition” [i.e. enjoying thinking hard and problem solving], greater curiosity, and open-minded thinking.
In the journal Self and Identity, the results from a study by Porter and Schumann (2017) suggest that intellectual humility can be increased in individuals through a growth mindset of intelligence; hence we could all benefit from intellectual humility in our lifetime development. The authors concluded that “teaching people a malleable view of intelligence may be one promising way to foster intellectual humility and its associated benefits.”
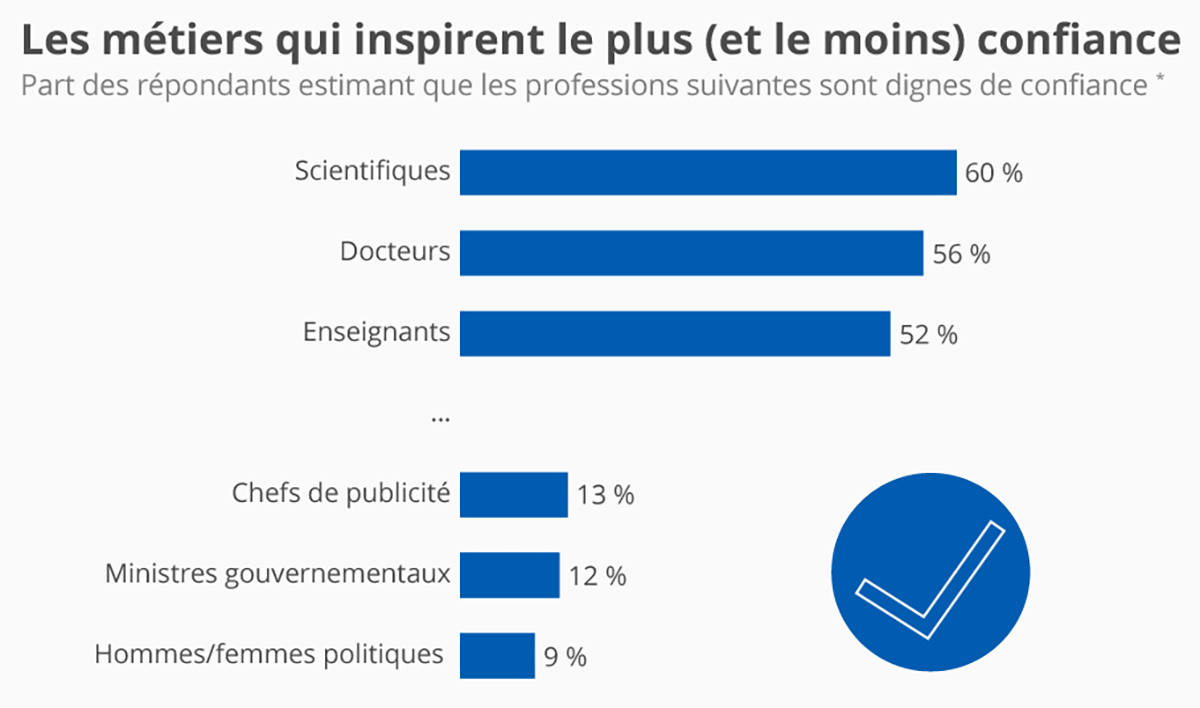
Les métiers qui inspirent le plus (et le moins) confiance / Source: Statista France
Many uncharismatic, simple-minded, grotesque and mediocre politicians need to acknowledge that their lack of knowledge, creativity and cultivation makes their ambitions of leadership impossible, and also understand that the ancient and stagnant political structure with parties and group agendas as it is nowadays can be considered as a discipline that is dead-alive and on its last leg; that hardly elicits the passionate interest of the civilised crowd anymore. The politics of parties and division is ongoing for the simple reason that civilised society has not yet implemented an organised and sophisticated concept to replace it and use it to manage our modern and interconnected human civilisation.
Regarding the degraded and cheap form of politics around the world in the 21st century, people at large need to firmly understand that every time typical, plain and ignorant office workers stack enough money aside to be able to afford quitting their day job in order to join a group of politicians in a movement, it does NOT suddenly transform them into a superior authority that requires everyone to stand in line to listen to everything that comes out of their mouths; they cannot and will never win a noble and sophisticated philosophical debate by insulting and disrespecting intellect and science simply because it does not always conform to their wishes and is often against their disconnected and backward outlook, while also at times being too challenging for most of their average, limited, naive, unproductive, boring and uncreative brains.

Traduction(EN): « An elite psychology theorist who deals with brain behaviour and sculpture at the granular level will not listen to the absurdities of a simple mind, even if the partners of this simple mind can pay all the advertisers in the world to publish their nonsense on toilet paper, cereal boxes, the cheap animal press to bus stops. We are above that! Every time a drugged out publisher of an obscure corner of the Internet creates a title with an image he considers degrading, it has no effect on us, none, zero; with his sweaty, sticky fingers slamming on a dirty keyboard on the 10th floor of an old building in a crowded corner of a polluted urban jungle? we are above these little defamation campaigns organized by childish politicians and the Jewish media they love so much. It cannot be anti-semitic to simply state that the majority of the press is owned, and hence controlled by Jews. My message to these people is this: « Try to grow up! Not a single intelligent person in the world is defined by your impulses… you are worse than children. People define themselves… simple….. your opinions, they’re just simple opinions as simple as your mind! » -Danny J. D’Purb
So, these simple animalistic minds and parvenus in the media along with those who hold their leash in politics need to seriously understand that no matter how many rotten tomatoes they throw at the wall of reason, these bricks were built on science, philosophy and intellect, and they will NEVER go down; to explain this logic, we can use the example, of the scientific facts that alcohol consumption and smoking cause cancer, and that flesh in a state of decomposition is a breeding place for maggots. Quite clearly, no amount of headlines, photo editing or covers will ever change those facts and convince any intellectually cultivated mind otherwise – although that does not seem to stop some cheap, corrupt and deluded media businesses and journalists from trying – the marketing of Trump by the media is an equivalent example. We all know that some people are hired to do so, but they would make their own lives easier and less stressful by knowing the limits of rational possibility, that is, by understanding the simple logic that covering gold with manure and swine scum will never transform it into those.

Image: Un alcoolique / An alcoholic
During the CoVID-19 pandemic, these haters of intellect and science then insisted on something as serious as a vaccine – that science cannot provide on demand – as if it was as simple as feeding or mass breeding pigs on a farm. As Holden Thorp also noted, for the past 4 years the obese Trump and his circus made deep cuts in the scientific budget including cuts to funding for the Centers for Disease Control and Prevention and the NIH. For their selfish political goals, the grotesque administration’s disregard for the science of the Environmental Protection Agency and the National Oceanic and Atmospheric Administration, and stalled naming of a knowledgeable director for the Office of Science and Technology Policy has caused a lot of harm over 4 years to US residents and the credibility of the US itself on the world scene.
Then, with the devastation caused by CoVID-19, Trump suddenly needed the discipline he disrespected and ignored, i.e. science. Yet, to cite Thorp, « the centuries spent elucidating fundamental principles that govern the natural world—evolution, gravity, quantum mechanics—involved laying the groundwork for knowing what we can and cannot do. The ways that scientists accumulate and analyze evidence, apply inductive reasoning, and subject findings to scrutiny by peers have been proven over the years to give rise to robust knowledge. These processes are being applied to the COVID-19 crisis through international collaboration at breakneck, unprecedented speed […] the same concepts that are used to describe nature are used to create new tools. So, asking for a vaccine and distorting the science at the same time are shockingly dissonant. »
The website PubPeer.com allows users to comment on scientific articles in post-publication, but also to report suspicions of breaches of scientific ethics. The site highlighted gaps in several high-profile articles, which in some cases led to retractions and accusations of scientific fraud as noted by the blog RetractionWatch.com, which analyzes retractions of scientific articles and comments on issues related to scientific integrity. PubPeer exists because of the inability of some hard empirical science to sometimes replicate its results and effectively self-correct itself.
A reliable vaccine must have a strong scientific foundation and will have to be manufacturable and safe. To achieve this, it has taken some time, and although the top scientists have been working as fast as they can to deliver this life changing vaccine, we could not have expected a miracle in instantly [e.g. in 3 weeks]. The business executives from those giant pharmaceutical companies who see life in terms of bank notes, had every thing to gain in getting the vaccine fast but luckily for people, even they also understand that we could not have used magic to get there in a week. However, we can perhaps take a positive note from this tragedy, since a couple of years ago Trump declared his skepticism about vaccines and even tried to launch an antivaccine task, but then crippled with COVID-19, he suddenly now loves vaccines.
Herbert Holden Thorp beautifully said it: « If you want something, start treating science and its principles with respect. »
The Centers for Disease Control’s worst-case scenario suggested that about 160 million to 210 million Americans will be infected by December 2020; as many as 21 million will need hospitalisation and between 200,000 and 1.7 million people could die within a year. Harvard University researchers believe that 20% to 60% of the world’s population could become infected, and estimated that 14 million to 42 million people could lose their lives.

Une disparité qui pose question : les hommes meurent plus du #COVID19 que les femmes malgré le fait qu’ils aient été contaminés à part à peu près égale. Dans certains pays, cette différence est particulièrement marquée / Source: Statista France
As Ian Goldin also suggested, the extent to which excess mortality can be prevented depends on how quickly societies can organise itself medically and culturally to reduce new infections, isolate the sick and manage health services and resources humanly and efficiently, and also on how long relapses can be prevented and contained.

La France compte rattraper son retard sur les #tests et a fait du #dépistage massif son fer de lance pour lutter contre le #covid19. Voici un état des lieux du nombre de tests réalisés par habitant dans une sélection de pays / Source: Statista France
While intelligent campaigns that teach and reshape human cultures on hygienic habits to deal with viruses may help, without a reliable and effective vaccine and an intelligent vaccination campaign along with systematic organisation, rapid manufacture and delivery, COVID-19 will remain as a hugely disruptive force for years, the pandemic will inflict more suffering and damage on poorer and most vulnerable communities within many countries, highlighting the risks associated with rising inequality.

COVID-19 : quel est le statut des cas identifiés ? / Statista France
In the US, over 60% of the adult population suffers from chronic disease, around 1 in 8 Americans live below the poverty line, and more than 75% of them live from paycheque to paycheque, and over 44 millions in the US have no health coverage at all; and to make matters even worse, they also constitute the largest culture of obesity and community of fat people on the planet.

Speaking with the Conversation France, Frédéric Altare, the director of the département d’immunologie at the Centre de Recherche en Cancérologie et Immunologie Nantes-Angers confirmed that being overweight is the major comorbidity associated with severe forms of Covid-19, which require admission to resuscitation in hospital. It can be estimated that, in some places, up to 80% of these may be related to obesity and that if we take a national average, obesity certainly accounts for more than half of the proportion of people admitted to intensive care. The fact that obesity creates a bias in favour of worsening the disease is also confirmed by the outbreak of the epidemic in the United States, a culture of hot dogs and big bellies where almost 40% of the population is severely obese. Since we are on the topic of hot dogs, a review of evidence in the British Medical Journal found that all processed meats [e.g. sausages, bacon, ham, and corned beef] are highly carcinogenic, i.e. they cause cancer, those foods all now appear in the same risk group for cancer (group 1) as asbestos, cigarettes and alcohol (Kmietowicz, 2015).

Le graphique présente les taux d’obésité (IMC>30kg.m-2). La moyenne des pays de l’OCDE est de 19,5% d’obèses. Les Etats-Unis, le Mexique, la Nouvelle Zélande et la Hongrie sont les pays les plus touchés avec respectivement 38,2, 32, 4, 30,7 et 30% d’obèses. Le Japon, la Corée, l’Italie et la Suisse sont les pays les moins touchés avec 3,7, 5,3, 9,8 et 10,3% d’obèses. La France est à 15,3% de taux d’obésité (donnée OCDE basée sur du déclaratif légèrement inférieure aux résultats d’ESTEBAN, basé sur des mesures) / Source: Centre de recherche et d’information nutritionnelles (Cerin)
This association between obesity and severe forms was already well-known for other respiratory infections such as the avian flu. The people at higher risk are those who have passed the morbid obesity milestone. Whether an individual is overweight is assessed using the famous « body mass index« , or BMI [You can check your BMI here], which is the ratio of weight to height squared. A person with a BMI above 25 is considered to be slightly overweight. From 30, we speak of proven overweight with the onset of obesity, at 35 we begin to speak of severe obesity, and from 40 we enter into what is called « morbid » obesity. Morbid, because the people concerned are considered to be at risk of developing pathologies, mainly cardiovascular and atherosclerosis, but also type 2 diabetes, liver diseases, certain forms of cancer.
The challenges to deal with the COVID-19 epidemic are also dramatic in Latin America, Africa and South Asia, where health systems are weaker and governments are less able to respond, risks caused by the failure of politicians such as Bolsonaro and Modi to take the issue seriously enough, argued Ian Goldin of Oxford University and Robert Muggah from the University of Rio de Janeiro.
In poor communities where many individuals share a single room and depend on day to day work to feed themselves, social isolation is difficult and around the world as individuals lose their income, we should expect rapidly rising homelessness and hunger. In the US, a record of 3.3 million people have already filed for unemployment benefit, and across Europe unemployment is also reaching record levels. Yet, in richer countries some safety nets exist even if they are struggling to organise themselves, but poor countries simply do not have the capacity to ensure that no-one dies of hunger.

Image: Une femme sans-abri tient dans ses bras son fils de 2 ans dans l’une des villes de tentes de Seattle / A homeless woman holds her 2-year-old son at one of Seattle’s tent cities Source: Business Insider (France)
All responsible and realistic governments around the world should therefore ensure that all people in need have a basic income to ensure that no-one starves as a result of this crisis. Goldin rightly observes that the COVID-19 pandemic provides a turning point in national and global affairs, it shows our interdependence and also that the general public tends to rely on governments to protect and save them and not the private sector, thus badly organised governments lead to human disasters… a song that most people are already familiar with.
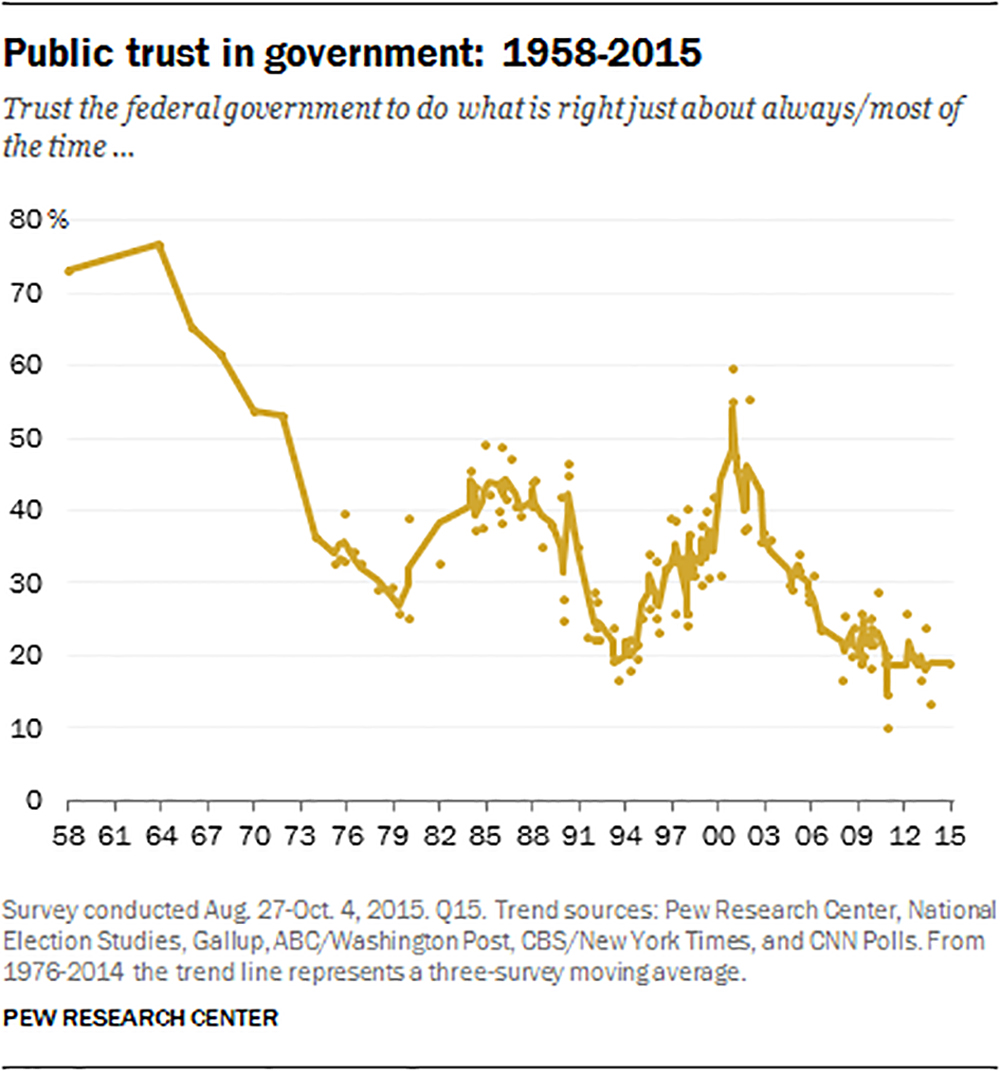
In agreement with my own suggestions, Goldin and Muggah also argue that at a time when faith in democracy is at its lowest point in decades, deteriorating economic conditions will contribute to even more political and social instability. There is already a tremendous trust gap between politicians and citizens.
Some politicians are sending mixed signals and citizens are receiving conflicting messages; this reinforces their lack of trust in public authorities controlled by politicians. Due to a shortage of international leadership from the US government, cities, businesses and philanthropies are stepping up.

Bill Gates delivers a speech at the fundraising day at the Sixth World Fund Conference in Lyon, France, on October 10, 2019. At the head of his foundation, Microsoft’s founder, wisely advocates international cooperation against the virus. (Photo by Nicolas Liponne/NurPhoto)
With the range of serious viral infections that have blighted the world during the last decades, it was only a matter of time for others to appear; most perceptive minds probably knew, but unfortunately these minds are a minority on our planet. « What’s to stop some form of SARS showing up? » Bill Gates asked in 2014, referring to the 2002-2003 epidemic of severe acute respiratory syndrome, caused by another coronavirus. Next, he said, could be « SARS II. » Bill and Melinda Gates established their foundation in 2000 and have always focused on biomedical innovations against disease and ways to deliver them. In 2014, during the Ebola epidemic that killed thousands worldwide, the Foundation was active in helping to stamp out the virus.
Governments should also take notice that the way a society cares for and treats its residents reveals a lot about their philosophy and their values about human life and dignity. As a modern civilisation, free high standard healthcare for all should be one of the priorities for all sophisticated and civilised societies, because people do not go to the hospital for fun, freebies or to collect free candies but end up there in situations of distress. Whether the public hospital has a homeless person, a high-earning lawyer, a student or a child at their doorstep, the quality of medical care should be at the highest standards for all, and societies who want to set an example to the world should certainly start with healthcare, because caring for the population is not spending but investing – a population in good health leads to progress at multiple levels [i.e. physical and brain development, educational achievement, psychological health, professional performance, etc]. Research and medical advancement are sectors that no government should discriminate because it ensures a healthy and progressive society.
Bill Gates in 2016 met Trump in the Manhattan skyscraper where the Trump Organisation is based and wanted to discuss « science and innovation ». Gates who co-chairs Bill and Melinda Gates Foundation – which is focused on infectious disease research and treatments – told Trump before he took office that he ought to make preparedness for the danger posed by viral pandemics a priority of his administration. But, of course, with Trump’s ignorance and lack of sophistication these words probably did not register on his brain who now says that « nobody could have predicted » the CoVID-19 virus » when Bill Gates did warn him. The only horribly stupid question that a scientifically illiterate Trump asked Bill Gates during that meeting was whether there’s « a difference between HIV and HPV ». Gates later recounted: « I was able to explain that those are things that are rarely confused with each other.”
“I feel terrible,” Bill Gates says now. And, “I wish I had done more to call attention to the danger,” even if it is the government’s responsibility to keep itself well informed and protect its population. Gates and his charitable organisation have so far committed more than $300 million to various coronavirus relief efforts, which is about 3 times the contribution of the whole of the US to the World Health Organisation.
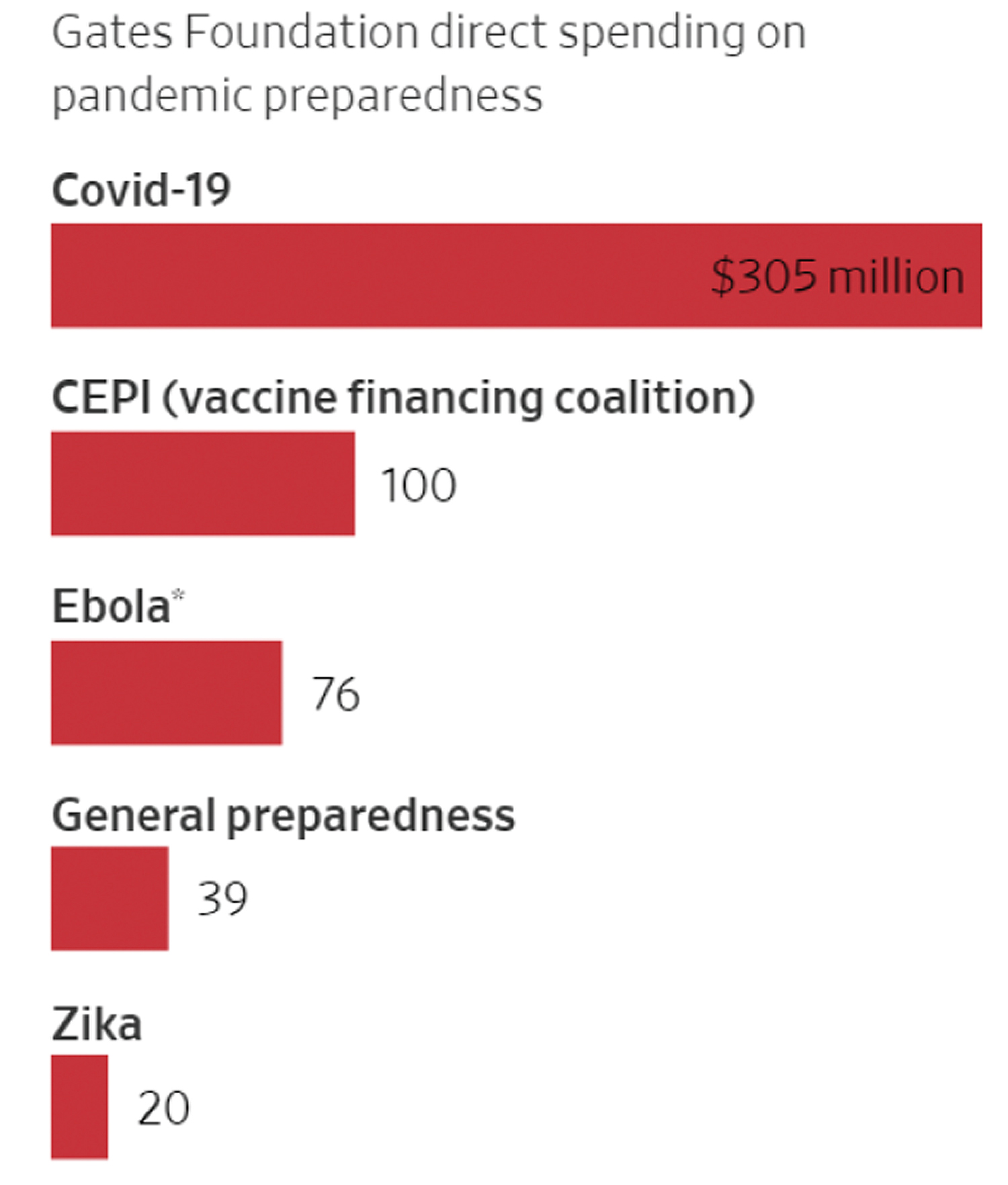
Gates Foundation direct spending on pandemic preparedness / Source: Bill & Melinda Gates Foundation
The point he made to Trump back then is more or less the same one he’s been stressing for years, including during a much-touted 2015 TED Talk in which he described viruses as posing the “greatest risk of global catastrophe.” “If anything kills over 10 million people over the next few decades, it’s most likely to be a highly infectious virus rather than a war,” Gates said at the time. “Not missiles, but microbes.” As of now the US is the global epicentre of the COVID-19 pandemic with more than 29 millions cases confirmed and 543, 000 deaths according to the Johns Hopkins COVID-19 resource center, exceeding the 58,220 lives lost over nearly 2 decades in the Vietnam war.
The Bill & Melinda Gates Foundation have invested $100 million to fight the new coronavirus in China; Twenty million will go to institutions including the World Health Organization (WHO), the American and Chinese Centers for Disease Control and Prevention, and the National Health Commission in China. Twenty million will be allocated to public health authorities in sub-Saharan Africa and Southeast Asia, areas that have been disproportionately affected by recent epidemics including the H1N1 pandemic in 2009. Up to $60 million will be spent on research into vaccines, treatments and diagnostic tools. Other groups such as the Wellcome Trust, Skoll, the Open Society Foundations, the UN Foundation, and Google.org are also scaling up assistance.
It is clearly not the appeals to atavistic and extremist nationalism and closed borders that will trigger solutions and make the most out of the complexities of our interconnected global civilisation in times of crisis where coming together as one planetary civilisation with a unified economic, scientific and medical force is key to destroying this virus and also prepare for the next epidemic; the solution is not about closing the borders or opening the borders, but to create a strong, safe, reliable and intelligent filtration system that is also flexible, reasonable and humane to people and allows movement in and out that contributes to the multi-layered forms of development of a country and civilisation as a whole (e.g. intellectual, academic, educational, linguistic, literary, artistic, cultural, scientific, medical, technological, economic, etc), through the transmission of connaissance (knowledge) and savoir-faire (know-how).
If those who feel that they have the responsibility to shape our human civilisation read and fully understand the essay, “Psychological Explanations of Prejudice & Discrimination“, they should come to realise what the theory of evolution is about; scientifically there is no such thing as a « pure » race [because all human primates on earth are the product of migration, breeding and evolution]. The theory of evolution formulated by Charles Darwin revealed to mankind that there is no stable and eternal essence, and that any idea of an exceptionally pure entity that would be beyond evolution does not exist – everything on our planet is in a constant state of flux/change [so from a scientific, evolutionary and organic standpoint, racism is a totally archaic absurdity since we are all simply organic matter on a small blue planet in the vast universe being recycled, recreated and reshaped in a continuous process]. Darwin stated very clearly that he honestly thought that evolution is accepting the idea that there is no end to evolution and it goes in all directions. The French philosopher Barbara Stiegler wisely suggested that the task of creating the consent of the masses should be left in the hands of experts in psychology [i.e. those who understand the psychic structure and philosophies of how humans and societies operate, develop and evolve].
Ian Goldin and Robert Muggah agree on the idea that the spread of COVID-19 must be met with a coordinated international effort to find vaccines, mobilise medical supplies and, when the volcanic dust settles, to ensure that we never again face what could be an even deadlier disease. They write on the University of Oxford’s Oxford Martin School website : « Now is not the time for recriminations: it is the time for action. National and city governments, businesses, and ordinary citizens around the world must do everything they can to flatten the epidemic curve immediately, following the examples set by Singapore, South Korea, Hong Kong, Hangzhou and Taiwan. »
Bill Gates remains optimistic about the crisis, since COVID-19 will allow the world to accumulate experience and prepare for the next pandemic. The modern and forward-thinking philantropist believes that the innovation shown by countries in the northern hemisphere could be of great help to countries in the south that are likely to be affected by the virus in the coming seasons, Gates is convinced that the fight against the virus requires a more realistic count of the number of proven cases, the Microsoft founder will finance the free distribution of testing tests in his city of Seattle. For him, the coronavirus could be the epidemic of the century. In practice, as soon as the tests are available, they will be distributed on demand in Seattle. The aim is that anyone with symptoms will be able to make the diagnosis themselves, by rubbing a cotton stick into the back of their nostrils. The Foundation says it can quickly process thousands of tests every day and deliver results within 48 hours maximum. Positive screenings will be notified to the patients, as well as to public health authorities. Positive patients will then be asked to complete an online questionnaire to detail their recent travels and the people they may have been in contact with. The aim is to better monitor the epidemic and to ensure that potential patients do not travel to hospitals or doctors’ offices.
“You can’t get ‘outside », said Professor Didier Sicard, who also argues for a universal attitude, which comes at a right time to educate world culture on medical hygiene, « We must not consider that we are 30 years old and in good health and that we are not going to be fooled by all this talk. » Everyone must realize that they may be unknowingly contaminating others. The epidemic has passed through people who have returned from China or Italy. Didier Sicard says: « I know the example of an Italian woman who went to Argentina. She attended a wedding and kissed everyone. This woman infected 56 people! Irresponsibility in times of epidemics does immense damage. On the contrary, we have to respect the measures. Like waiting, for example, in front of the supermarket before entering if you see that there are people. »
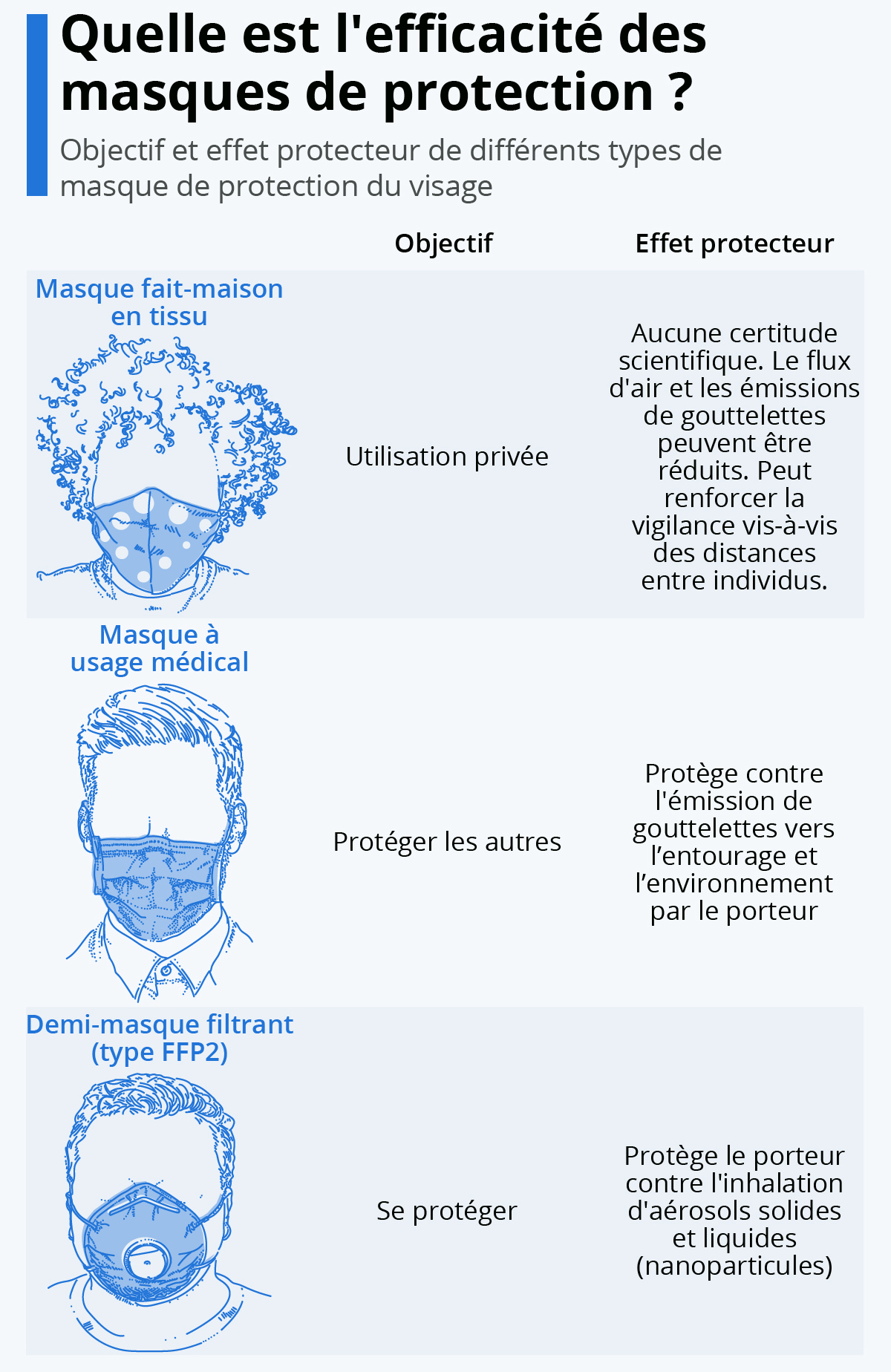
Quelle est l’efficacité des masques de protection ? / Source: Statista France

Où les masques sont déjà omniprésents: le gouvernement a annoncé que des masques seraient distribués aux Français / Source: Statista France
Surgical face masks have been proven to significantly reduce the detection of influenza virus RNA in respiratory droplets and coronavirus RNA in aerosols, with a trend toward reduced detection of coronavirus RNA in respiratory droplets, hence surgical masks have the potential to prevent the transmission of human coronaviruses and influenza viruses from symptomatic individuals (Leung et al., 2020).
Until the world population is immunised, the face mask will become the indispensable and essential accessory for us all at all times, when we are in environments frequented by others. Most popular among lay people, the cloth mask is already being widely used and it is re-usable; this accessory will be the key to ease us all out of lockdown and offer some temporary protection to us and the people around us. THE MASK IS NOT A MIRACLE PROTECTION, SO INDIVIDUALS MUST REMAIN VIGILANT AND NEVER LOWER THEIR GUARD and are advised to seriously take notice of where their hands and fingers are going and ensure that it does not get in contact with their face [i.e. mouth, eyes, ears], carry a hand-sanitiser with at least 60% alcohol with them at all times and use it properly, maintain a safe distance of about 1 metre minimum from all other individuals at all times, and also stay away from those who are not wearing masks as micro droplets from their breath and mouth may contaminate others.

A study published in the PNAS using highly sensitive laser light scattering showed that micro droplets generated by asymptomatic carriers of COVID-19 during speech can emit thousands of oral fluid droplets per second and these can remain in the stagnant air of confined environments for up to about 15 minutes. This confirms that there is probability that normal speaking causes airborne COVID-19 virus transmission in confined environments (Stadnytskyi, Bax, Bax and Anfinrud, 2020).
People should also not be ashamed about their appearance due to protective measures, nothing is enough for a deadly virus, and I would personally recommend using safety goggles that completely seal the eyes when outdoor in highly frequented public places such as shopping areas. People should also never lose their focus about the possible sources of contamination indoors, such as shoes and clothes worn outside. It may be life-saving to organise a specific routine such as leaving shoes worn outside in a corner, sanitise hands when touching them. Perhaps as soon as one gets home, instantly remove and place all clothes worn outside in a basket far from people in the house, outside in a sheltered place may be convenient for washing then disinfect oneself and shower.
We must NEVER FORGET that there is a deadly virus circulating and any minor slip or even a small reflex [e.g. scratching the eyelids] can mean death. The Académie de Médecine recommends the facial mask for all.
How to maintain your cloth mask

Image: Scorpion of Mortal Kombat may motivate the younger generations to wear their masks and maybe even the more mature generations
There are many people who do not know that the cloth mask MUST COVER THE NOSE AND THE MOUTH otherwise it would be pointless, hence it is advisable to tell any person not wearing their mask properly to do so; the mask should also not be used for more than 4 hours. Generally, the cloth mask must be washed every time that it has been used, taking into consideration that usage should not exceed 4 hours. Hence, it is obvious that every individual will need to have a few in order to rotate them during the day appropriately.
The Association Française de normalisation (Afnor) also advises to wash this protection every time it is dirty or wet or badly positioned on the face. To be worn properly, the mask must cover the nose and the mouth and should not be placed in waiting position on the forehead or around the neck. The Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM) also stated that all mask makers must give details on how to wash and disinfect their masks. Here is a list of some helpful advices for an optimal maintenance:
- Wash at 60 degrees celcius with your usual laundry for at least 30 minutes preferably in the machine, or if not available, by hand
- Dry the mask in the 2 hours that follow the washing in a dryer, or if not available, with a hair dryer
- At the slightest sign of wear (e.g. hole or deformation) the mask must be discarded.
Here are also a few things that you MUST NOT DO:
- Place it in a microwave
- Iron it without washing it
- Use bleach or alcohol
- Dry it in open air

Before the wash
Before the washing process, the Afnor precisely explained in its FAQ that it is not necessary to systematically disinfect the inner tube [i.e. the area that holds the laundry] before washing your masks. However, Afnor recommends to run an empty wash if you have accidentally added a used mask with other clothes during a wash at a temperature lower than 60 degrees celcius. In this case, we must proceed, before the wash, with a cold rince of the inner tube with bleach, or run an empty wash in the machine at 60 degrees celcius or 95 degrees celcius without spin.
During the wash
Masks should be washed with your usual detergent at a temperature of 60°C for at least 30 minutes in the washing machine or, if this is not possible, by hand. The use of fabric softener is not recommended. It is best not to use any product other than your usual detergent, as any other product could degrade the mask fabric. Furthermore, the Afnor specifies that you can wash your masks with sheets or towels, in order to « ensure the mechanical aspect of the wash ».
The Drying Process
The Afnor believes that « the mask should be completely dried within the two hours that follows the washing« . Whenever possible, the mask should therefore be tumble dried after cleaning the filters. Drying in the open air is slower, but it can be an alternative, » we find on the Afnor website.
Can the mask also be blown dry? The option is mentioned in a standard notice for fabric/cloth masks put online by the Direction générale des Enterprises. But Afnor does not recommend this method, because of the « poor control of the temperature level », which can lead to damage to the fabric. If you nevertheless choose this option, for lack of any other solution, it is therefore essential to pay attention to the temperature supported by the mask. The ANSM also recommends, if possible, steam ironing the mask. This can help to complete the drying process, adds the Afnor. Here again, be careful with the temperature so as not to damage the fabric or the elastics.
Whichever option you choose, all layers of the mask must be completely dry. As a final step, before storing it in a clean, airtight package, visually inspect the mask. If you notice any deterioration (wear, deformation, holes, etc.), discard the mask.
If Washing Is Not Possible
It is not recommended to microwave the mask. Steam ironing or hair drying is not a substitute for washing either. Finally, it is absolutely not recommended to use bleach or alcohol to disinfect a mask. Not only can these two products alter the quality of the mask by degrading the fabric, but bleach is also dangerous to your health (with risks of skin irritation or respiratory problems).
The Stop-postillons site, created by doctors, nevertheless gives this advice, if one cannot disinfect one’s mask right away: « keep it in an airtight box (for example a plastic box disinfected with bleach) », then « wait a week ». You can also find a simple method to make your own mask that does not require any additional material except a pair of scissors and a t-shirt.

Image: Comment fabriquer votre propre masque en utilisant un t-shirt et une paire de ciseaux [Cliquez pour regarder la vidéo] / Source: stop-postillon.fr
On masks, Didier Sicard declared: « …they are psychological protectors for walkers and not virological protectors. Every French person has to say to themselves: I do everything so that others can’t blame me for anything. We need an attitude where we look for the other’s gaze before our own. That alone will bring efficiency. Masks are obviously protective for doctors and caregivers in an environment where the virus circulates. But when you have people walking down the street wearing masks, it’s paradoxical. They think they’re protecting themselves from others, but there’s a huge gap between the uselessness of masks on the street and the vital usefulness of masks in hospitals. I myself was at the pharmacy on Saturday morning and I showed my doctor’s card to see if I could buy masks. The pharmacist told me there were none left. So, if I needed them to treat a patient, I wouldn’t have been able to go see him, or I might have contaminated him. We have seen too many people walking down the street wearing masks as a kind of panoply. There is a major political drama in this absence of masks.”
Sicard pointed out that masks should be reserved for carers, stating: “To anyone who works around the virus. When you see cashiers at the supermarket who don’t have masks while customers have masks, there is something completely counterproductive. Those who don’t need them have got them, and those who really need them are missing them. This is directly related to individual behaviour. I would never have dared to walk down the street with a mask until the caregivers had masks. It’s something that would have frightened me. It basically shows people’s blindness and ignorance. If you walk around without meeting anyone, there is no point in wearing a mask.”
Didier Sicard
From an ethical standpoint, the attitude of carers who are now on the front line when they were on strike a few weeks back struck Sicard, who said: “That’s their duty. A doctor is mobilized in his inner self to do his job. Cowards don’t come at the beginning. So, it seems both admirable and normal to me. The suffering of the hospital body, I’ve been seeing it for ten or fifteen years. The number of my colleagues who have told me, you are so lucky to be retired! We suffer, it’s terrible, the hospital has become a business. And I totally agree with what they said: the hospital has been martyred. With purely economic decisions that ignored the interests of patients and doctors. The number of doctors who took early retirement should be measured by explaining that their profession no longer had any interest and that they felt they were spending their time filling in forms and boxes. There has been a real ransacking of the public hospital over the last decade. The last Minister of Health who was still really aware of his role and who respected health care workers was Xavier Bertrand. After that, it was a disaster.”
Sicard also did not think that this broken health system had any repercussions today faced with the current sanitary crisis in France, adding: “All the measures that made the hospital non-functional have temporarily disappeared. The administrators are terrified in their offices and do nothing. The doctors are doing everything. They have regained all their power.

There is a certain happiness for them in finding the job they always wanted to do. The administration has packed up its bags, or more precisely, it is in charge. The balance of power has been reversed: a year ago, doctors were at the orders of the administration; now, it is the administration that is at the orders of the doctors. This is a very interesting phenomenon. Doctors themselves are no longer hindered by being forced to fill the beds with patients who bring in money, which was the principle until then. Now they’re going back to their core business. Which is the fight against death. Deep down, they find the deep DNA of their craft. It’s almost a paradox: there is less distress in the medical profession now at peak activity, than there was six months ago when they were desperate and depressed because they felt that their profession had lost its meaning.”
Sicard seems to rightly observe and believe that the politicians will remember this period and that civilisation is changing era: “I can give you an example for which I’ve been fighting for two years. I won’t name the hospital, but I know a woman who specializes in burn surgery. At the hospital, her department was closed and she didn’t have a position anymore. Nevertheless, she wanted to continue working with children with burns. However, her burn unit was transformed into a plastic surgery unit for buttocks and breasts. Because it brings in a lot of money. But she always tells me that if there was a fire in a school with forty or fifty burned children, we would no longer have the capacity to take them in because we consider that burns are not profitable enough and that it is better to focus on surgery for the stars. »

Où perd-on foi dans le capitalisme ? / Source: Statista France
« This economic vision of medicine, which has been introduced over the last ten years, is an absolute disaster, » declared the experienced medical professional This was of course a public hospital, “In the private sector, institutions do what they want. However, it is not normal for the public sector to destroy an activity that is not profitable – because burns are very expensive and bring in very little money and there is no private activity capable of dealing with them – and to dismiss it in favour of profitable activities. Basically, the public was anguished at the idea that it had to invest heavily in top-of-the-range equipment to match the private sector. The public will never have as much money as the private sector and will never be able to keep up. And by spending money on highly specialized sectors, we end up neglecting the most vulnerable people, be they the elderly, alcoholics or people in precarious situations. The public hospital has ended up forgetting its hospital function, as I have said on several occasions. Ninety per cent of doctors have been aware of this and it has been a terrible suffering for them. Just as it was for nurses and other care workers to do a job that was linked to money.”
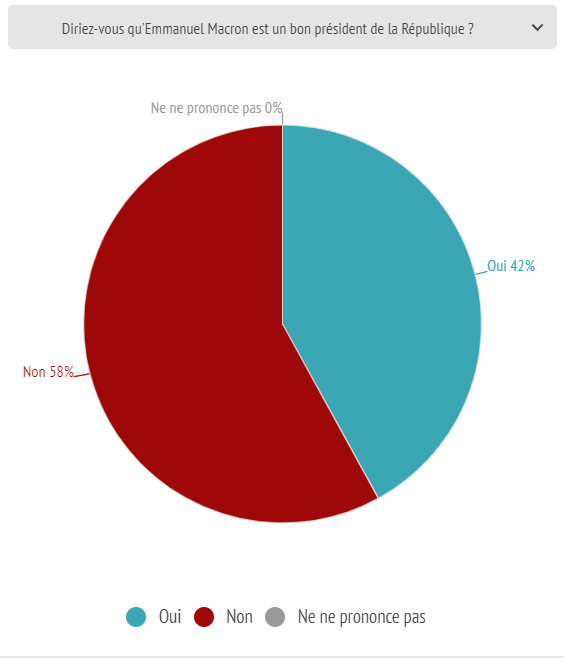
La majorité des Français pensent que le Macron banquier est inutile comme leur président / Source: Odoxa
Professor Sicard believes that we have no assurance that politicians will change their views on health care, however he thinks that the French will remember and will hold them to account, saying: “President Macron had promised to stop activity-based pricing, the current system of hospital financing. Economists have been pushing the envelope, saying that we would no longer be able to measure the cost of this or that operation. And the head of state gave up. I think that after this crisis, the President of the Republic will modify this activity-based pricing. The hospital will ask to be reimbursed on what it achieves and what it considers its priority. We have to trust the hospital not to treat patients unnecessarily and fill beds as if we were at the club méditerranée. The hospital will regain its true public care function.”

Image: Médecin scolaire au travail en France / School doctor at work in France
In the UK, at Oxford University, researchers have been working with Oxford University Hospitals NHS Foundation Trust to reduce clinical research activity to allow researchers to prioritise research on COVID-19 and to support the pressing clinical needs of the NHS. The academic community will have to work together with governments, funders and healthcare providers to combat this ugly COVID-19 virus and Oxford has a long history of responding to health emergencies, e.g. during the 2014 Ebola crisis among negro communities in Africa, Oxford scientists lead the way in undertaking human vaccine studies, and Oxford’s strength in research around infectious diseases and international health, alongside its leading work in emergency vaccine development places it in a great position to contribute to better comprehension around the effective control of this horrific epidemic.

Source: Oxford University Research
The Oxford team had already tested a potential coronavirus vaccine successfully on several animal species. The World Health Organisation (WHO) had reported that over 70 vaccines were being developed globally for the COVID-19. The Oxford team joined 3 other groups of researchers, 2 in the US and 1 in China for the start of human trials. Professor Sarah Gilbert, a vaccinologist at Oxford University said she was « 80 per cent » confident it will be a success. Patrick Vallance, the UK’s chief scientific adviser said that it would be « very lucky » if a coronavirus vaccine was available widely within a year.

Image: Researchers at the laboratory of British pharmatech company Exscientia at Oxford Science Park in Oxford, part of an initiative to develop coronavirus treatments. Source: Adrian Dennis/AFP via Getty Images
The Oxford group are among the most advanced viral vaccine group in the world and have been working on vaccine preparedness for several years which means that they have been able to test and evaluate Covid-19 vaccine candidates rapidly. The group have unique unique viral vector delivery and expression systems combined with diverse expertise from basic virology to vaccine production scale-up.
The UK has no current vaccine manufacture however, and may have to rely on its Western European neighbours (e.g. France, Belgium and Germany) that have industrial level manufacturing capabilities. The Jenner Institute and Oxford Vaccine Group, could develop a jab that would be ready as early as September, almost a miracle in speed for such a demanding task as people are dying by the thousands every couple of hours globally.

COVID-19 CORONAVIRUS PANDEMIC Live Counter (here last updated on March 24, 2021) / Source: Worldometer (Click to see the live counter)
So, we are going to need a technology that allows us to deliver billions of doses over a year. The team at the University of Oxford said that they expect to produce a million doses of their experimental vaccine as early as September; months ahead of the official 12-to-18 month timeline quoted by experts around the world. “Then we’ll move even faster from there, because it’s pretty clear that the world is going to need 100s of millions of doses ideally by the end of the year to end this pandemic and let us out of lockdown safely”, said Professor Adrian Hill, Director of the Jenner Institute, University of Oxford.

Part des Français prêts à accepter des mesures de quarantaine afin d’endiguer la propagation du nouveau coronavirus (COVID-19) en France en 2020 / Source: Statista France
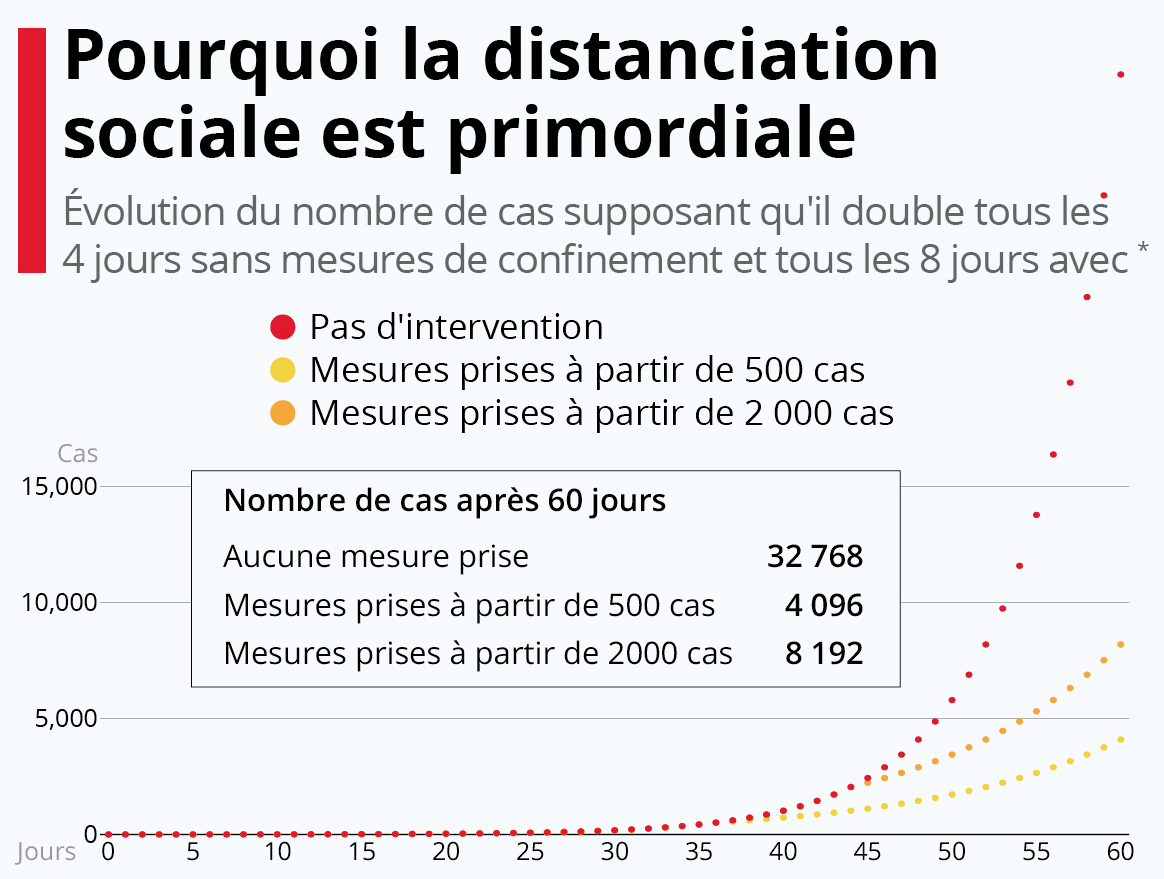
Pourquoi la distanciation sociale est primordiale / Source: Statista France
The Oxford University team’s experimental product, called « ChAdOx1 nCoV-19 », is a type of immunisation known as a recombinant viral vector vaccine and was just one of at least 70 potential Covid-19 candidate shots under development by biotech and research teams around the world. The vaccine had been chosen as the most suitable vaccine technology for the virus as it can generate a strong immune response from one dose, said the team. When they were asked how they managed to move the usually lengthy process of vaccine approval along so quickly, Professor Sarah Gilbert, lead the study, said it had been their ongoing research into Disease X – an as yet unknown infectious agent earmarked as a potential pandemic in the making – which has allowed them to pivot so quickly to COVID-19.

Traduction(EN): « I am in no doubt that we will see an unprecedented spirit of collaboration and cooperation. » – Sarah Gilbert
We should be looking into creating a planetary medical organisation that is minutely planned and efficiently organised around the latest and finest technological advancements. All vaccine researchers and developers worldwide have a responsibility towards mankind to synchronise their knowledge and findings in the development of the ultimate vaccine.
The World Health Organization will also have to prioritise works on the linguistic synchronisation of planet Earth’s medical worlds since this unification of the medical talents and expertise worldwide is of upmost importance for the future of mankind and civilisation. What we mean by linguistic synchronisation is that the whole medical community will need to work in one language as it will speed up development, and will also be one fundamental cornerstone towards building a united planetary civilisation, even if individuals are free to learn or study other tertiary languages if that is what they desire, such as being a member of particular societies [e.g. book clubs, ancient languages of civilisation, etc]
It is important to emphasise that in this essay, my usage of the terms “united planetary civilisation” is very different to “globalisation”, since the latter term is vague and generally refers to labour, migratory movement and financial motives, whereas the “building of a united planetary civilisation” is about getting humans of earth to genuinely agree on values and goals, feel, understand and synchronise their lives with each other as a truly united planetary community that is helping, working and building harmoniously together at every level and not only economically.

Carte montrant la différence des niveaux de littératie entre la génération plus âgée et la plus jeune / Map showing the difference in literacy levels between the older and the younger generation / Source: OurWorldinData
We are after all living in pivotal times where the human civilisation is evolving at breakneck speed and changing era right before our eyes in the 21st century with a generation that has the chance of having access to the wide range of accelerated learning technologies available; the world’s societies have evolved beyond recognition from their « primitive » past, and are today interconnected and inspire and influence each other in so many ways [e.g. science, sport, medicine, cuisine, arts, literature, philosophy & education].

It is also to be noted that with all the difficulties that the delicate intellectual responsibility and duty to shape and structure the construction of a modern civilisation involve due to the lack of sophistication, open-mindedness, personality along with the persistent culture of atavism of many rigid, naive, ignorant, infantile and petty little minds, especially in the Anglo-Saxon sphere, reminding me of a comedic post about the 29 things French people love about Britain, but more particularly in the even more savage industrial and mechanical wild west of the US.
As a bilingual Franco-British individual with native mastery of French and English, I have always invested my time and energy in the cause of mankind’s evolution and tried my best to act as a cultural bridge between the academic, medical, scientific, intellectual, psychological, philosophical, and psycholinguistic realms of the 2 most widely spoken languages in the so called « developed world » – that sometimes unfortunately still feels like concrete jungles through the savage behaviour, actions and reasoning of some passionless and unsophisticated creatures that are supposed to set an example, inspire, motivate, guide a civilisation and create a humane and harmonious society where « le dépassement de soi » is a realistic pursuit and where individuals can grow in multiple ways, truly « live » in the full sense of the term and not simply have a plain and meaningless existence where achievement is purposeless and devoid of sense.
In our times, however, there are still many regions of the world that are linguistically « undeveloped »; where the majority cannot even master simple communication in English, let alone grasp the finesse, artistry, romanticism, emotional sensibility, humane values of the enlightenment, sophisticated philosophy, and depth of the psychical realm of literary French.

Traduction(EN): « Can anyone tell me how a simple female monkey with electrodes, let alone a (so-called) minister of culture, can talk without dying of shame about a « learning » summer?
I repeat: a learning summer.
A summer, therefore, that learns.
That learns what?
To write French, no doubt. » / Source: Twitter (Juan Asensio)
Indeed, just like the great majority of useless, cheap, uncultivated and frustrated street politicians in France, the great majority of their political counterparts in other parts of the world also fail to do so, unconsciously suffering from a lack of literature, self-cultivation, artistic exposure, self-respect and dignity combined with a constant complexe d’infériorité towards those who are wiser, smarter, nobler in spirit, more intelligent, creative, charismatic and sophisticated than them; I would recommend them to sit down and listen to the university lectures of Prof. Michel Butor [E.g. Les récits philosophiques de Balzac], it may help towards their cultural evolution, but also ease the pain on those forced to endure them, such as their wife and children.
Honoré de Balzac (1799 – 1850)
It is time for them to firmly understand that we still have some « adultes surdoués » as Monique de Kermadec » phrases it, or « Overmen » as Friedrich Nietzsche puts it i.e. highly talented and skilled individuals who live and exist out there, especially in the psyches of the French speaking world and heritage [e.g. Napoléon, of whom even the great German Georg Wilhelm Friedrich Hegel himself described seeing as follows: « I saw the Emperor – this world-soul – riding out of the city on reconnaissance. It is indeed a wonderful sensation to see such an individual, who, concentrated here at a single point, astride a horse, reaches out over the world and masters it. »]; individuals who have the savoir-faire and creative power to manage dozens of governments worldwide, a film/video/music/media production company, a publishing house, who could also give a lesson in professional artistic photography, post-production and presentation, and even train a whole generation of original, sophisticated, witty, poetic, literary and noble writers, and not just in Oscar Wilde’s granular Oxford English, although flat compared to French, but also « la langue Française de Balzac » in all its precise articulations, depth, style and literary artistry.

Image : La Cité des Mots (City of Words), par Vito Acconci (1999)
Logically, to such individuals, running a press/publishing/media business would be a piece of cake, something achievable half-asleep with superior values, style, efficiency and impact than the mass of mediocre newspapers and their usually obese owners and political sympathisers out there; if such a direction was a career choice and goal for those gifted individuals at a particular point of their life – of course!
Besides, my whole life I have questioned my own sanity because I have always felt misunderstood and different from the rest of the crowd and highly sensible and receptive to what most primates around me could not even hear, sense, feel, see, perceive or understand, and also never found anyone in the Anglo-Saxon realm with a mastery of French similar to mine, and nobody in the French realm with a mastery of English as mine, thinking that I could be fake, I then realised that linguistic discourse and speech are not fake, but are very real and alive, as Jacques Lacan also concluded.
Luckily, I recently read Monique de Kermadec’s book « L’Adulte Surdoué » and found out that humanity has a minority of individuals out there in the world who also feel misunderstood and are hard to classify, because just like myself, these « weird fools » and misunderstood individuals have an IQ of above 145 [which I only recently found out myself from a small IQ test on the MENSA website that only measured up to 145, which is sufficient for me to know without an exact number since this is a statement of fact not an exercise of arrogance – delivering me from my torment to confirm that the weird ones are not us, but the mediocre majority that surrounds us and cannot follow our discourse or understand our lightning speed judgements because of their lower IQ – valuable things in nature are rare, that is why they are valuable]. That is genuinely valuable knowledge for individuals out there among the human population who may also have felt or feel the same way. It is known that around 2.5% of the human population fit the classification of “Surdoué” or “Haut Potentiel”.

Graphique montrant la répartition de la population humaine en fonction du QI // Chart showing the distribution of the human population according to IQ
While 2.5% may not seem a great proportion, it still amounts to around 197 million [196 874 145] people on earth from a population of 7.9 Billion [7 874 965 825]. It is highly recommended for those individuals to learn about their singularity and channel their talent appropriately because human civilisation needs the contribution of those amazing individuals for its betterment. There are books written by some experts who have dedicated their career to these amazing individuals. Intellectuals such as Nathalie Clobert who studied individuals who fit the description of “Haut Potentiel”, who also tend to come with the trait of “hypersensibility” [i.e. they are more receptive to almost any stimuli and so, they feel more, sense more, understand more and are more reactive]. Clobert’s book “Psychologie du haut potentiel: Comprendre, identifier, accompagner” responds to the need for training and information of professionals by offering a reference book on the subject. The book covers the major aspects of the theme of the “Haut potential”: from the reference models of giftedness to the accompaniment of children and adults, including current scientific research, identification and differential diagnosis issues. She made an appearance on France Inter in 2021 to discuss the HPI (Haut Potentiel Intellectuel), in a discussion entitled “Comment fonctionne le cerveau des enfants et des adultes surdoués, à haut potentiel intellectuel ?“
Jeanne Siaud-Facchin is also another trusted name in the study of those particularly gifted individuals; her books “L’enfant surdoué, l’aider à grandir, l’aider à reussir (2002)“, “Les Surdoués (2004)“, and “Trop intelligent pour être heureux ? L’adulte surdoué (2008)” provide some essential reading on the matter for individuals out there who may be looking for some light in the dark tunnel of the amazing “Haut Potentiel” or as parents to gifted children. Jeanne Siaud-Facchin founded the Cogito’Z centres and dedicated her career to understand the particularities of these singular profiles who are the scouts of tomorrow’s world, giving particular attention to their power of thought, their sharp analysis, their exacerbated lucidity, their intuition and creativity, their hyper-connected brain, their hypersensibility, their exacerbated emotions, explaining that those are strengths to which these incredible individuals can relate to in order to shine and feel at home in the face of the complexity of a disoriented world.
Siaud-Facchin also posts videos online and educates employers and professionals about the need to understand those particular indiviuduals and their superior abilities in order to make the most of such potential in the professional world and also to allow those individuals to succeed at multiple levels; a more direct way to word it, is that those readings will give employers and professionals a better understanding of the ways to manage, deal and/or interact with individuals who are more intelligent, smarter, faster and more creative than them.

Hence, from the perspective of someone who fits the category, it comes across as a responsibility to other gifted individuals and civilisation to point out that most superior individuals with superior intellect will not see the majority constituted of cold-blooded, cannibalistic, reptilian political primates as a model to follow, as an inspiration, as a source of comfort, safety, hope or stability, as a spiritual guide or as an ultimate authority, but instead just see them as a bunch of other boring, cold, disconnected and mechanical bureaucrats; artistically, culturally and philosophically poor souls, and divisive money-minded & party-oriented politicians with simple minds, passing by, like the thousands of mediocrities who have lived and died before them and who have been responsible for some of the most castastrophic human disasters in history without ever being able to accept their mistakes.

Traduction [EN]: “Men make mistakes, great men confess that they have made mistakes.” – Voltaire
When we look back, we also find that those unscrupulous party-oriented bureaucrats have not had any major positive impact on the world; and are at this minute rotting in a forgotten grave with maggots sliding through their bones. While, my self-respect and moral fibre prevents me from doing such a disgraceful and disrespectful act, it comes across as hard for me not to think of the title of Boris Vian’s book, “J’irai cracher sur vos tombes”.

Image: Benoit Ferreux lisant « J’irai cracher sur vos tombes » de Boris Vian dans le film Le Souffle au cœur, réalisé par Louis Malle, sorti en 1971.
We could even ask ourselves whether some of those disconnected bureaucrats – who mostly spent a few years amassing money in some mundane office, chatting in front of a coffee machine before joining a group of people who all see life though the same lens [i.e. left, centre or right] known as a political party – have green blood? It may be a sensitive and humane gesture of compassion to simply try and imagine the horror and agony it must be for any woman, who for whatever reason, has had to, or is having to wake up next to one of those reptilian primates every morning, with its eye lids slapped on a greasy face and in the centre of it, a mouth half open drooling on a pillow with its « haleine de boudin ».

Le gouvernement a-t-il été à la hauteur de la situation ? / Source: Odoxa
And to stress the point that most of the mediocre politicians nowadays cannot be trusted with the heart of the people, the historical and legendary verbal whipping from the great Napoleon himself to the evil, lying, sly, dishonest, disloyal and backstabbing politician, Talleyrand, who was plotting against the emperor with Fouché in 1834, comes to mind; looking at the untrustworthy face and straight in the eyes of the unscrupulous man, the emperor Napoléon said:
« Vous êtes un voleur, un lâche, un homme sans foi. Vous ne croyez pas à Dieu ; vous avez toute votre vie manqué à tous vos devoirs, vous avez trompé, trahi tout le monde […] Tenez, Monsieur, vous n’êtes que de la merde dans un bas de soie. »

Traduction(EN): « You’re a thief, a coward, a man of no faith. You do not believe in God; all your life you have failed in all your duties, you have deceived, betrayed everyone […] Here, sir, you are nothing but shit in a silk stocking. » – Napoléon (to Talleyrand, during the Council of Ministers convened at the Château des Tuileries) / Source: L’Histoire en Citations
Nowadays with the adaptive and dynamic technology and skilled software engineers available, we should be creating a sophisticated planetary medical system where the latest findings, empirical studies, analysis and statistics of the medical experts of the whole world are instantly synchronised and available in one place [with instant full-access to all medical journals worldwide], while respecting the personal and non-medical details of patients by a tested and proven system of indexing that does not allow for personal details to be input but only strict medical/scientific details. It may also be useful to note that when it comes to health problems, we are all equal on our small and interconnected planet Earth, and in the essay on clinical psychology, « Learning Disabilities, Anxiety, Depression & Schizophrenia and the Effectiveness of Psychotherapy », the global statistics portray this fact.
We should be focusing on specialised and highly encrypted [an encryption specially devised for this system that is 100% safe so that even if there are hacks and data breaches, the data will never be usable due to the powerful encryption] servers only accessible through highly controlled card systems, only available to the medical departments of hospitals and universities from all around the globe.
Such a system would speed up development for both medical professionals and patients. For example, If a patient suffering from cervical, skin, ovarian, testicular or lung cancer in any part of the world (e.g. Rio de Janeiro, New York, Moscow, Port-Louis, Mumbai, Tokyo, Alabama, Berlin, Jerusalem, Ottawa, Cape Town, Zurich, London, Grenoble or Paris) has a CT scan, that scan would be instantly uploaded and classified in the medical database on the specialised and encrypted servers and made available to all medical departments and professionals in the world connected to the system, who would then have the options to add comments or questions, with their involvements being rewarded by points.
The heads of medical faculties at universities could even have the option to use these live data and cases to train medical students, and in doing do, provide a revision to the diagnosis and treatments of patients while also subjecting the cases to constructive criticism and/or new treatments being developed.

Image: Étudiante en médecine en formation / Medical student in training
A similar scenario could also apply for all diseases and all types of treatment that would be minutely and systematically classified while remaining intuitive to browse, sort by a range of variables and access for medical professionals; the age, blood group, weight, height, sex and other medical details only would be made available on the specialised server, not private non-medical information. Such an advanced system would not only connect the medical community, stamp out medical negligence and raise medical standards, but also provide a massive dataset from which a range of institutions could carry medical research and have a more precise conclusion from statistical tests. From the essay on clinical psychology, “Controversies that surround modern day mental health practice“, we clearly pointed out a range of different views among the medical community on a range of controversial treatments; such a system would lead to a more open-minded debate among the academic community on ethics and methods of treatments while considering individual patient characteristics across different fields of medicine and treatment.
This system with a well organised database could also be used to manage a global blood bank and ensure that it is evenly distributed internationally so that even those with rare blood groups can be treated efficiently when health problems arise;

Image: Un serrurier au travail / Locksmith at work
for example, if the daughter of a motel owner, fried chicken and hot dog seller in Illinois happens to be of a very rare blood type and she finds herself in desperate need of it to remain alive, she could instantly have access to the rare blood which could have been collected from the other side of the globe and extracted from the veins of a locksmith in Amiens, an aborigine in New Zealand, a noodle seller in China, a dwarf circus-performer from an English village, a banker in India, an Eastern European stripper in Las Vegas, a heavy truck driver in Madagascar, a kangaroo keeper in Australia, a potato farmer in Germany, a gay bouncer and bodybuilder in Austria, an old and bald Breton who edits a low class « plouc » newspaper in Northern France, a retired, frustrated, useless and senile politician in Brazil, a peasant with a limited vocabulary and a strong « Marseillais » accent, or a globally known elite, bilingual French writer, intellectual, philosopher, thinker, speaker and creative artist – because such an efficient and sophisticated system would allow for a systematic management of blood banks globally.

Image: Don de sang / Blood donation
That system would also include the profiles of medical professionals accessible between them along with a system of forums, awards, points and chats where any medical department and expert could post messages regarding the recruitment of patients for studies, the latest findings of particular medicines and treatments from the wide range of departments and specialities; and also the top articles from scientific journals made available by different departments – until we work on such a sophisticated system, humanity will continue to suffer from a lack of organisation and management.
A system as sophisticated and organised as that would lead to the world being up-to-date and synchronised medically, with patients also receiving the latest treatments or having the option to travel to different parts of the world for new treatments against deadly diseases or terminal stages that are still in the trial phase and also doctors remaining focused and sharp through the latest updates in their specific fields while also giving them the ability to instantly ask questions on the forum/chat to other experts in their fields right from the operating table if they are unsure or would like some words of support or confirmation.

Image: Microsoft Teams, un exemple de modèle pour une application collaborative / Confinement: le nombre d’utilisateurs quotidiens a augmenté de 12 millions en l’espace d’une semaine. Le 11 mars, Microsoft Teams comptait 32 millions d’utilisateurs quotidiens, pour ensuite voir ce chiffre passer à 44 millions le 18 mars / Source: Statista France
They may even have a live camera streaming system on their foreheads or face while conducting surgery so that it can be seen by all those connected to the system in private clinics, hospitals and the medical faculties of universities worldwide. Such a system could be regulated by an independent global medical authority that would also deliver certifications to all institutions and professionals who apply for it, patients could also see a particular logo on their treatment locations to see that they are part of such a system; if this is implemented even minor hospitals in small villages will suddenly have the boost and expertise of the top medical experts behind them. This would lead to an instant rise in medical standards worldwide.

Image: Une femme en France discutant avec son médecin / A woman discussing with her doctor in France
In the 21st century with the affordability of powerful multi-core processors, high-definition audiovisual equipment and high speed broadband it is a scenario that is very realistic and not a far-fetch scene from one of the infantile mass produced science-fiction fantasies of the Hollywood industry.
We need to apply the technological ingenuity of mankind appropriately to make the most of our lives in this world and allow our fellow humans to live more and stress less, and not simply focus all that technological prowess into creating brain numbing and absurd entertainment media and other petty devices and apps that lead humanity to a culture of mundane, mediocre, meaningless and useless social blogging and nonsense, where bored and pathetic people share photos of their sandwiches, drinks, breakfast and make-up tips with the world.
From an article in the Lancet, Sarah Gilbert said: « WHO is in the process of creating a forum for everyone who is developing COVID-19 vaccines to come together and present their plans and initial findings. It is essential that we all measure immunological responses to the various vaccines in the same way, to ensure comparability and generalisability of our collective findings. Work is continuing at a very fast pace, and I am in no doubt that we will see an unprecedented spirit of collaboration and cooperation, convened by WHO, as we move towards a shared global goal of COVID-19 prevention through vaccination”.

Chart: The twelve SARS-CoV-2 vaccine candidates reaching/announcing Phase III clinical trials by mid-November 2020. Shown in pie-chart configuration are the companies responsible for the development of the vaccines, the technology each vaccine uses, their reported efficacy in Phase III trials. *, efficacy not yet available. Due to variability in reporting criteria for cases of COVID-19, efficacy results may not be directly comparable. (Funk et al., 2021)

Table: Avantages et désavantages des différentes plateformes vaccinales / Advantages and disadvantages of various vaccine platforms (Loo et al., 2021)
I also take the opportunity to salute all the medical teams and healthcare workers operating all over the world for the courageous task they are undertaking and also express all my gratitude and support to my local NHS GP surgery in West London who have always been there when I needed them and who are still texting their patients to show their concern and support in these difficult times affecting the entire human civilisation.

« This is a snapshot of the message I received from my local GP surgery in West London on Friday, 10th of April at about midnight (UK time) even if I am out of the UK at the moment after more than 14 years without taking any holiday or leave of absence from the country. My plans to return in January with a trip to Oxford has been ruined by this ugly Coronavirus pandemic, and now all the flights have been frozen… my heart remains and will forever be in Western Europe. » -Danny D’Purb
On this note, the British psychoanalytical Society have set up “With You in Mind”, a consultation in times of crisis to support NHS and social care staff who are working and are under immense pressure while being exposed to risk during the COVID-19 pandemic. Members of the Institute of Psychoanalysis, who are all mental healthcare specialists are volunteering their time to offer support sessions. These volunteers are hoping that the opportunity to talk may offer some relief and support – whether about professional or personal matters, or the situation at work, they are hoping to help in any way they possibly can.

With You in Mind: Consultations in Crisis
Psychoanalysts can also support reflective practice activities [they can be contacted by CLICKING HERE or if you are a member and would like to find out more, email: support@iopa.org.uk]
Steps to prevent infection are vital:
There are many things we can do to protect ourselves and the people we interact with. As with a cold, a flu vaccine won’t protect people from developing COVID-19. The best thing we can do at this point is to follow the same preventive measures as we would against the flu. It is widely known that individual can catch the flu when people sneeze and/or cough on them, or when they touch a dirty [infected] doorknob. We should wash our hands thoroughly especially before eating or touching the facial area and cavities and also after using the bathroom, while also avoiding others with flu-like symptoms – these are the best strategies for the time being.

Déjeuner d’un employé de bureau âgé à Londres / Elderly office worker in London having lunch
The following preventive actions are also recommended:
- Wash hands with soap and water for at least 20 seconds. Dry them thoroughly with an air dryer or clean towel. If soap isn’t available, use a hand sanitizer with at least 60% alcohol.
- Stay at home if sick.
- Avoid touching nose, eyes, and mouth. Use a tissue to cover a cough or sneeze, then dispose of it in the trash.
- Use a household wipe or spray to disinfect doorknobs, light switches, desks, keyboards, sinks, toilets, cell phones, and other objects and surfaces that are frequently touched.
- It may also be important to create a household plan of action. You should talk with people who need to be included in your plan, plan ways to care for those who might be at greater risk for serious complications, get to know your neighbours, and make sure you and your family have a household plan that includes ways to care for loved ones if they get sick. This includes planning a way to separate a family member who gets sick from those who are healthy, if the need arises.
- Medical professionals recommend that people voluntarily wear cloth face masks in public settings where other social distancing measures are difficult to maintain, including grocery stores and pharmacies, especially if they live in an area of significant community-based transmission. It should be noted that the cloth mask is not meant to protect the wearer from infection. It is instead meant to slow the spread of the virus (if people who have the virus and do not know it wear masks, they help prevent transmitting it unknowingly to others). Health experts advise making face coverings at home from simple materials, and reserving surgical masks and N95 respirators for health care workers and other medical first responders.
While everyone should take precautions, measures may be critical for adults over 65 years old (the risk seems to gradually increase with age starting at age 40, according to the World Health Organization) and those with chronic conditions (such as diabetes, heart disease, and lung disease).

Les plus de 70 ans, principales victimes du #COVID19 pourraient être confinés plus longtemps / Source: Le Parisien
People in these higher risk categories especially should stock up on household items, groceries, medications, and other supplies in case they need to stay home for an extended period of time. The world also faces another crisis, which is the risk of a toilet paper shortage as the COVID-19 crisis has slowed down the delivery of goods, and most notably those of paper pulp.

#Consommation : les Français se seraient-ils montrés plus raisonnables que les autres face à l’achat-panique ? On peut se poser la question au regard de cette estimation de la hausse des ventes de #papiertoilette par pays en mars / Source: Statista France
Steps to follow if you become infected and fall ill:
Until now, information available shows that the severity of COVID-19 infection ranges from very mild (sometimes with no reported symptoms at all) to severe to the point of requiring hospitalisation. Symptoms can appear anywhere between 2 to 14 days after exposure, and may include:
- Fever
- Cough
- Difficulty breathing
Getting in touch with one’s medical provider for advice in the eventuality of experiencing these symptoms, especially if you have been in close contact with a person known to have COVID-19 or live in an area with ongoing spread of the disease is recommended.
Most people will have a mild illness and will usually be able recover at home without medical care. Seek medical attention immediately if you are at home and experience emergency warning signs, including difficulty breathing or shortness of breath, persistent pain or pressure in the chest, new confusion or inability to arouse, or bluish lips or face. This list is not final, so consulting your medical provider if other concerning symptoms are noticed is vital.
François Sureau : « Les Français ne sont pas un troupeau de moutons ou une garderie d’enfants »
To conclude, just like Goldin and Muggah, I also believe that the major Western European players, China, Japan and especially France, a world leading and cultivating nation, must set an example for history by stepping up and leading a global effort, forcing the deteriorated and unstable US government and the uncharismatic politicians controlling it into a global response, which includes accelerating vaccine trials and ensuring free distribution to the world once the ultimate vaccine and antivirals are perfected and finalised. Governments and financial institutions around the world will also need to take dramatic action toward massive investments in health, sanitation and basic income and also provide financial support to both struggling employers and employees.
Potential treatment for those infected with COVID-19
For those who have been infected, as already explained above, we have some studies suggesting that convalescent plasma [i.e. donated blood from people who have recovered since this donor blood has antibodies to COVID-19] lead to shorter hospital stays and lower mortality for patients who received the treatment while no severe adverse effects were observed (Chen, Xiong, Bao and Shi, 2020). It has also been shown that chloroquine, hydroxychloroquine and tocilizumab have the potential to act as a potential cure in « some » patients but they are not guaranteed to function in all cases of COVID-19. Remdesivir was approved in the US to treat COVID-19 in patients who are ≥12 years old and weigh at least 40 kg. This antiviral drug is able to prevent the viral genome of SARS-CoV-2 from replicating. TOCILIZUMAB has even recently shown to cure COVID-19 patients with severe underlying medical conditions; it has cured a patient who recently had a kidney transplant (Fontana, et al. 2020), and others with asthma (Schleicher, Lowman and Richards, 2020), systemic sclerosis (Distler, 2020), multiple myeloma (Zhang, et al. 2020) and sickle cell (De Luna, et al. 2020).
Some doctors in France are claiming to have healed patients infected with CoVID-19 through the use of antihistamines, a well-known and easily accessible medication against seasonal allergies, and some patients are claiming that in 24 hours their symptoms disappeared [i.e. blocked nose, runny nose, aches and pains]. Although no empirical studies have been carried out yet, these French doctors are claiming that since antihistamines can reduce inflammation in its early stages it can prevent progression towards dangerous stages. Dr Hélène Rezeau-Frantz prescribed antihistamines to 18 patients who were symptomatic but untested and after a couple of hours they all started feeling better. These doctors are claiming that antihistamines carry no risk of serious adverse effects and genuinely believe that we may be on an interesting trail towards treatment and are asking for serious studies to be carried out on antihistamines.
All these recent advances have been referenced below in the « Références (Études Scientifiques) » section, and academics & medical professionals are kindly urged to read, analyse and continue further research in this direction and the world can also help by spreading this information as far and wide as they can without wasting a single second.
Potential Protection against COVID-19: Vaccines
For those who are not infected and suffering from the severe symptoms of the COVID-19 virus, the best form of protection is vaccination. Throughout humankind’s history, vaccinations have played a significant role in eradicating diseases and improving public health since the discovery of the smallpox vaccine by Edward Jenner in 1796. Vaccines are administered to a host [a patient] to produce an immune response similar to that produced by a natural infection without resulting in a diseased state. The purpose of introducing a vaccine to the host is to produce immunity and an immunologic memory like that of a natural infection. Hence, if the host is exposed to a natural infection in the future, their immune system will be able to elicit an immune response to fight against that infection.
As mentioned earlier, the S protein on the SARS-CoV-2 virus plays an essential role in allowing the virus to bind to and enter the host cell. It enables the virus to attach to host cells via receptor recognition and triggers a cascade of events contributing to its pathogenesis. The S protein has vital functions that makes it a target in developing a vaccine. A range of vaccines have been released and vaccination campaigns have started around the planet with at-risk age groups being given priority. Researchers have developed various types of vaccines with the release of the genetic sequence of the SARS-CoV-2 virus in January, and all those vaccines reach their optimal efficiency after 2 doses; these include inactivated viral vaccines, protein sub-unit vaccines, mRNA vaccines, and recombinant viral vector vaccines, with the 6 most popular ones being:
(i) ChAdOx1 nCOV-2019 Vaxzevria produced by the University of Oxford/AstraZeneca
(ii) Gam-COVID-Vac Sputnik V produced by Gamaleya Scientific Research Institute
(iii) mRNA-1273 produced by Moderna
(iv) BNT162b2 produced by Pfizer & BioNTech
(v) NVX-CoV2373 produced by Novavax
(vi) BBV152 Covaxin produced by Bharat Biotech

6 Pricipaux Vaccins: (i) ChAdOx1 nCOV-2019 Vaxzevria produced by the University of Oxford/AstraZeneca; (ii) Gam-COVID-Vac Sputnik V produced by Gamaleya Scientific Research Institute; (iii) mRNA-1273 produced by Moderna; (iv) BNT162b2 produced by Pfizer & BioNTech, & (v) NVX-CoV2373 produced by Novavax (vi) BBV152 Covaxin produced by Bharat Biotech
(i) ChAdOx1 nCOV-2019 Vaxzevria Vaccine produced by the University of Oxford/AstraZeneca
The ChAdOx1 nCOV-2019 Vaccine produced by the University of Oxford/AstraZeneca uses adenovirus-vectored technology [i.e. recombinant viral vector technology], a harmless, modified version of a common cold virus that usually spreads among chimpanzees. This altered virus may cause a person to become ill, but it carries a gene from the novel coronavirus’s spike protein, the portion of the virus that triggers an immune response; this allows the immune system to manufacture antibodies that works against COVID-19, hence teaching the body how to respond should it become infected with COVID-19. Recombinant viral vector vaccines are generally built upon a non-replicative virus or an attenuated replication-competent virus, which is bioengineered to express antigens from the target pathogen. Although various viral vectors are being studied in vaccine development, only a few recombinant viral vector vaccines have been approved for human use. (Loo et al., 2021)
The original strategy for the Oxford/AstraZeneca vaccine was to deliver a single-dose vaccine. However, it was found that two doses provided much better immune responses. It has been found that those who had a longer interval actually developed much better immune responses after the second dose; this has also been noticed with other vaccines, such as the one against cervical cancer. Longer intervals between the 2 doses provide better immune responses because the immune response matures after the first dose is administered. When it is given enough time to mature, a very good memory booster response is obtained when the 2nd dose is administered. If the 2nd dose is administered too early, the immune response will not have matured fully, so there is some negative feedback, and so it does not overshoot the mark, hence we obtain a smaller response to the 2nd dose (Mahase, 2021).
For the ChAdOx1 nCOV-2019 Vaccine produced by the University of Oxford/AstraZeneca, recent data backs a 12 week [3 months / 84 days] interval between the 1st and 2nd dose. That decision is based on an analysis from 3 single-blind randomised controlled trials involving 17 178 participants in the UK, Brazil and South Africa. The study found vaccine efficacy reached 81.3% after a second dose in those with a dosing interval of 12 weeks or more (95% confidence interval 60.3% to 91.2%). If those doses were given less than 6 weeks apart the efficacy would have been reduced to only 55.1% (CI 33.0% to 69.9%). These observations are supported by immunogenicity data that showed binding antibody responses more than two-fold higher after an interval of 12 weeks or more compared to an interval of less than 6 weeks. These findings confirm that the vaccine is efficacious with outcomes varying by dose interval with a 3-month interval being advantageous over a programme with a short dose interval for a pandemic vaccine to protect the largest number of individuals in the population as early as possible while also improving protection after the 2nd dose. A single standard dose of vaccine was found to provide 76% protection overall against symptomatic COVID-19 starting from day 22 to day 90 after vaccination, with protection not falling in this time frame. We cannot tell how long this protective first dose could last since too few cases were available after 90 days to reach any meaningful judgement. However, it is important to note that analyses suggest that it is the dosing interval and not the dosing level which has the greatest impact on the efficacy of the vaccine (Voysey et al., 2021). This is in line with previous research supporting a greater efficacy with longer intervals with other vaccines such as influenza and Ebola. Researchers found that the vaccine however appears quite poor at preventing asymptomatic infection although its efficacy increased with a longer gap between the 1st and 2nd doses (Wise, 2021).
In an earlier interim primary efficacy analysis conducted with 11,636 (7548 in the UK, 4088 in Brazil), a group of participants were not given the usual 2 standard doses, but were instead given a low-dose (2·2 × 1010 viral particles) as their 1st dose and were then boosted with a standard dose (5 × 1010 viral particles) as their second. An incredible efficacy of 90% was noted in those who received a low dose as prime, this was intriguingly high compared with other findings in the study. The researchers declared that this might be chance at play, however, exploratory subgroup analyses, included at the request of reviewers and editors, that were restricted to participants aged 18-55 years old, or aligned with an dosing interval of more than 8 weeks showed similar findings. Hence, the use of a low dose (LD) for priming could provide more vaccine for distribution at a time of constrained supply while, according to the data, also not compromising the protective effects. However, wide confidence intervals around those estimates conclude that further data will be required to confirm those preliminary findings (Voysey et al., 2021).
There has been some worldwide unfounded controversy regarding ChAdOx1 nCOV-2019 Vaccine produced by the University of Oxford/AstraZeneca where many citizens and healthcare workers have been rejecting it. This irrational hesitancy came after a German newspaper caused international upset when it claimed that the vaccine was ineffective in older people basing itself on just one single anonymised source without any evidence. The European Medicines Agency and many other countries however have ignored this claim and approved the vaccine for over 65s, including most recently, Canada. The Canadian drug regulator said that the vaccine’s efficacy in this age group was supported by factors outside clinical trials. Evidence came from a vaccine rollout to healthcare workers and elderly people in Scotland that showed how the vaccine reduced the risk of admission to hospital by up to 94%, four weeks after the first dose was administered (Torjesen, 2021). These findings may have prompted a change to the recommendations in France, where the ChAdOx1 nCOV-2019 Vaccine is now approved for adults up to 75, after originally being restricted to those under 65.
As it has proven to be effective and has an acceptable safety profile, ChAdOx1 nCOV-2019 Vaccine became the second vaccine to be approved in the UK and has been administered to prioritised groups first. The vaccine was also later approved for use in Europe and India [the Oxford-AstraZeneca vaccine is being produced under licence by Serum Institute India under the commercial name Covishield].
The adenoviral vector vaccine, ChAdOx1 nCoV-19 has also demonstrated efficacy against the B.1.1.7 (UK) variant which similar to the efficacy of the vaccine against other lineages. Vaccination with the ChAdOx1 nCoV-19 leads to a reduction in the duration of shedding and viral load, which may translate into a considerable impact in the reduction of disease transmission (Emary et al., 2021).
Other studies, released in a preprint, to further investigate the vaccine’s efficacy against the B.1.351 (South Africa) variant and the B.1.1.7 (UK) variant have been conducted on Syrian hamsters, which have been successfully used for the preclinical development of several vaccines including Ad26 vaccine by Janssen and mRNA-1273 vaccine by Moderna since those specific rodents have a SARS-CoV-2 infection model that is characterised by natural susceptibility to SARS-CoV-2 and the development of a robust upper and lower respiratory tract infection (Muñoz-Fontela et al., 2020). Animal models such as the Syrian hamster play an important part in science, for example, in the development and evaluation of potential chemotherapeutic agents against leishmaniasis; Syrian hamsters infected with Leishmania species lead to visceral leishmaniasis (VL) that closely mimic the disease in natural hosts, including target organs, lesions, and clinical course (Jiménez-Antón, Grau, Olías-Molero and Alunda, 2019).

Image: Le hamster syrien comme modèle expérimental avancé en médecine / Syrian Hamster as an Advanced Experimental Model in Medicine
With the ongoing evolution of SARS-CoV-2, the readily available and cost-effective Syrian hamster model allows rapid evaluation of the protective efficacy of novel VOCs (Variants of Concern). In addition, it will allow rapid preclinical benchmarking of existing vaccines against preclinical vaccines with updated antigen designs.
Those studies showed that ChAdOx1 nCoV-19 vaccine may be less effective at reducing upper respiratory tract infection caused by the B.1.351 (South Africa) than the B.1.1.7 (UK) along with reduced efficacy against mild disease; however complete protection against lower respiratory tract disease was observed, which is consistent with protection against severe disease. So, based on those results, the researchers hypothesise that the currently available vaccines will likely still protect against severe disease and hospitalisation caused by the B.1.351 (South Africa) variant. ChAdOx1 nCoV-19 vaccination resulted in complete protection against disease in hamsters and hence, viral vectored vaccines may provide substantial protection against lower respiratory tract infection caused by the B.1.351 variant and subsequent hospitalization and death (Fischer et al., 2021).
A study assessing the efficacy of the ChAdOx1 nCoV-19 Vaxzevria vaccine against the B.1351 (South Africa) variant published in the well known New England Journal of Medicine made a major mistake, which seems to suggest that researchers out there are missing some of the advances being made in vaccine efficacy or not exploring the wide range of journals. The study was carried out on 2026 participants and they were given 2 standard doses 21 to 35 days apart, and we know that the vaccine does not reach maximum efficacy if given less than 6 weeks apart, in fact with new data dosing gap must be at least 12 weeks. So, we can assume that the methods were wrong and the results have reflected the mistake (Madhi et al., 2021).
(ii) Gam-COVID-Vac Sputnik V Vaccine produced by Gamaleya Scientific Research Institute
The Russian vaccine known as Gam-COVID-Vac Sputnik V produced by Gamaleya Scientific Research Institute was developed and produced entirely domestically in Russia. In March 2020 when the COVID-19 had already been declared as a world pandemic by the World Health Organization, the Gamaleya National Center of Epidemiology and Microbiology in Moscow was already working on a protype of Sputnik V, funded by the Russian Direct Investment Fund (RDIF), the country’s sovereign wealth fund.
It is a recombinant viral vector DNA vaccine (i.e. the similar viral technology used by the ChAdOx1 nCOV-2019 Vaccine produced by the University of Oxford/AstraZeneca), except instead of using chimpanzee viruses, 2 common human cold viruses were used in the vaccine prototype; the vaccinologists opted for 2 different human adenovirus vectors (rAd26 and rAd5) delivered separately in 2 doses, 21 days (3 weeks) apart. Since using the same adenovirus for the 2 doses could lead to the body’s immune response to act against the vector and destroy it when the 2nd dose is administered, 2 different vectors reduces the likelihood of such a scenario.
The results of both Phase I and Phase II were published in the Lancet based on 76 participants, and according to the paper all participants developed SARS-COV-2 antibodies and no serious adverse effects were observed, at the exception of some mild ones [such as half experiencing pain at injection site] (Logunov et al., 2020). The interim phase III data for the Gam-COVID-Vac Sputnik V vaccine was published in early February 2021 which included 22,000 adults aged 18 years or older. The results indicate that the vaccine is 91.6% effective based on its ability to prevent symptomatic infection. Some 94% reported very mild side effects, and 4 deaths were recorded during the study which were not related to the vaccine (Logunov et al., 2021). The phase III data have been met warmly by the academic community. Russia has gone to great lengths to promote Sputnik V beyond its borders in a vaccine diplomacy drive, promising that it will cost les than $ 10 (£ 7.20; 8.40 Euros) per dose for international buyers.
The University of Oxford and AstraZeneca have even launched a trial to be held in Russia to assess whether mixing doses of their own ChAdOx1 nCOV-2019 Vaxzevria with the Gam-COVID-Vac Sputnik V may yield more benefits to patients worldwide. This initiative in based on the fact that effective vaccines usually require more than one time immunisation in the form of a prime-boost. Traditionally, the same vaccines are given several times as homologous boosts. Findings have suggested the prime-boost against a particular virus can be done with different types of vaccines containing the same antigens; in many cases such heterologous prime-boost can be more immunogenic than homologous prime-boost (Lu, 2009).
Scientists in Russia are also working on 2 versions of the initial Sputnik V vaccine: one that needs to be stored at -18°C, freezer temperature, and another that uses dried (lyophilised) material that can be stored at 2 to 8°C in a range of standard refrigerators, which would aid transport and distribution. Yet more versions of the vaccine are also in the works, including a single dose alternative.
While the vaccine seems to have a high efficacy, one of the main concerns about the safety of the product is the use of the Ad5 vector. According so some researchers who published an article in the Lancet, the use of a recombinant adenovirus type-5 (Ad5) vector may lead to an increased susceptibility to HIV infection among some men, hence they are suggesting to be cautious in using recombinant viral vector vaccines with Ad5 in areas of high HIV prevalence. It is important to clear out the confusion and prevent unecessary panic; the vaccine will not give the recipient HIV, since it is a virus that is transmitted from others. However, these researchers who worked with an Ad5 vectored HIV-1 vaccine (Moodie et al., 2015) about a decade ago are only suggesting to be cautious with the use of Ad5 vector since, if exposed to the HIV virus, it may increase the risk of developing HIV in some men [especially uncircumcised males] by lowering the immune response towards the HIV virus. According to the hypothesis put forward by those researchers, the immune response towards Ad5 induces a lowered activity of the CD4 and CD8 T cells which are specific to HIV. There is no solid data or studies to ascertain that the Russian Gam-COVID-Vac Sputnik V vaccine will lead to increased risk of HIV, but since only a few recombinant viral vector vaccines have been approved for human use, caution is being advised! Further research to dispel this risk would be most welcomed by all (Buchbinder, McElrath, Dieffenbach and Corey, 2020). South Africa, besides being the most severely affected country in Africa with COVID-19, is also a region where the prevalence of HIV is high [19% among adults 15 – 49 years of age], hence the Russian Gam-COVID-Vac Sputnik V vaccine has been placed under close observation there.
(iii) mRNA-1273 Vaccine made by Moderna
The mRNA-1273 Vaccine made by Moderna and the BNT162b2 Vaccine produced by Pfizer & BioNTech use a different technique to fight against COVID-19 than the ChAdOx1 nCOV-2019 Vaccine produced by the University of Oxford/AstraZeneca. These 2 former vaccines use a technology known as mRNA which does not use a virus DNA, but instead introduces a piece of genetic code (mRNA) that tricks the body into producing COVID-19 antibodies. mRNA vaccines had never been used therapeutically in human beings, this is the first time in human history!
Reseach has found that mRNA vaccines allow transient expression and accumulation of the target viral antigens, thus leading to a profound effect on the magnitude and affinity maturation of antibody responses, providing a longer duration of protection. mRNA vaccines are also non-infectious and non-integrating, this means a significantly lower risk of infection or insertational mutagenesis. mRNA is degraded in the body through normal cellular processes, and the 2 vaccines that use this technology [Moderna and BioNTech] rely on intramuscular injections to administer the vaccines since this prevents rapid digestion of the mRNA and avoids stimulation of the innate immune system which could lead to a reduced vaccine efficacy. (Loo et al., 2021)
The mRNA-1273 Vaccine made by Moderna data shows that a delay of at least 28 days between the 2 doses could maximise vaccination program effectiveness and prevent additional infections, hospitalisations and deaths. The interim analysis of Moderna phase III trial reported that the vaccine was 94.5% effective 14 days after the 2nd dose. The Moderna mRNA-1273 Vaccine can be stored at −20°C rather than the −75°C needed for the Pfizer/BioNTech vaccine, which makes handling it much easier. Moderna has announced that the vaccine can be kept in a conventional freezer for up to six months and that once thawed can be kept for up to 30 days in a standard refrigerator. This makes the vaccine much easier to deliver.
The most frequently reported adverse reactions to the Moderna vaccine were injection site pain, fatigue, and headache. Adverse reactions were usually mild or moderate and resolved within a few days after vaccination. The US Centres for Disease Control have reported that 29 people have so far developed anaphylaxis in response to being vaccinated with the Pfizer BioNTech and Moderna vaccines. It said the rate of anaphylaxis cases is currently around 5.5 cases per 1 million vaccine doses given [incredibly low]. In the decision documents, the MHRA tackled potential anaphylactic reactions. It said that “close observation for at least 15 minutes is recommended following vaccination” and advised healthcare professionals to ensure that “appropriate medical treatment and supervision to manage immediate allergic reactions” are readily available. (Mahase, 2021)
Regarding the B.1.1.7 (UK) variant of COVID-19, the preprints of a studies using the mRNA-1273 Vaccine that there was no significant impact on the vaccine’s neutralising ability against B.1.1.7 (UK) lineage. It has been found that both infection- and vaccine-induced antibodies were effective at neutralising the B.1.1.7 (UK) variant. However, reduced neutralisation was measured against the mutation present in the B.1.351 (South Africa) variant. The data resumed demonstrate that there was a reduced but still significant neutralisation against the full B.1.351 (South Africa) following mRNA-1273 vaccination (Wu et al., 2021; Edara et al., 2021).
(iv) BNT162b2 Vaccine produced by Pfizer & BioNTech
While very slightly inferior to Moderna’s performance, the BNT162b2 Vaccine produced by Pfizer & BioNTech is also mRNA based and succesfully averted more hospitalizations and deaths in the UK. The BNT162b2 Vaccine was found to have a 94% efficacy with a 3-week (21 days) dosing schedule between the 1st and 2nd dose. A published study assessing Israel’s vaccination rollout between 20 December 2020 and 1 February 2021 showed that 2 doses of the Pfizer-BioNTech vaccine reduced symptomatic cases by 94%, hospital admissions by 87% and severe COVID-19 by 92%. The paper also suggested that the vaccine was effective against the B.1.1.7 variant [the UK COVID-19 virus variant] (Wise, 2021).
However, the UK is the only country to have adopted a 12-week delay between the 2 doses of the mRNA based BNT162b2 Vaccine produced by Pfizer & BioNTech after recommendations by the Joint Committee on Vaccination and Immunisation (JCVI). This strategy is not in line with what the World Health Organization or the US Centers for Disease Control and Prevention who have both opted for the recommended 21 days (3-week) dosing delay (94% efficacy) and no more than a 6-week to the second dose in exceptional circumstances.
For the mRNA based BNT162b2 Vaccine produced by Pfizer & BioNTech, the 3-week dosing schedule was found highly effective in the phase 3 randomised clinical trial – regarded as gold standard. No clear advantage was found in delaying the 2nd dose of the BNT162b2 Vaccine produced by Pfizer & BioNTech in the reduction of infections, unless the efficacy of the 1st dose did not wane over time. An article in the Lancet questions the UK’s decision to go against the 3-week dosing schedule which is considered as gold standard. The UK’s Chief Medical Officers’ decision to adopt a 12-week delay is not supported by clinical data or efficacy generated from real-life clinical observational data from Israel (Chodick et al., 2021; Aran, 2021).
In the case of the ChAdOx1 nCOV-2019 Vaccine produced by the University of Oxford/AstraZeneca, the 12-week dosing strategy seems like a good decision since that vaccine is different, being DNA based and there is sufficient evidence to back the 12-week gap, but this is not the case for the mRNA based vaccins such as the BNT162b2 Vaccine produced by Pfizer & BioNTech. The JCVI made an assumption that the 89% effectiveness efficacy is obtained after the 1st dose. This estimate of 89% was obtained from an unplanned, retrospective analysis of the randomised clinical trial data, comparing COVID-19 cases in the vaccine group vs the control group from a 6-day window (15-21 days), selected retrospectively after examining the data; hence the 89% was based on about 20 events. Retrospective analyses in therapeutic trials can be used to generate hypotheses but should not be used to treat patients. So, without any solid empirical evidence, the JCVI made the major assumption that 89% effectiveness persists after the 1st dose from day 21 to day 85 in the absence of the 2nd dose [See: Chapter 14a & The Independent report of the Department of Health & Social Care]. In a further major incorrect assumption, the JCVI stated: “There is currently no strong evidence to expect that the immune response from the Pfizer-BioNTech and AstraZeneca vaccines differ substantially from each other”. The Pfizer-BioNTech vaccine is an mRNA vaccine different to the AstraZeneca DNA vaccine, and no scientific data on mRNA vaccines exists to support the JCVI’s assumption. The available quality peer-reviewed, published immunology data would refute the assumptions documented by the JCVI and Public Health England.
As already explained, mRNA vaccines have never been used before therapeutically in humans. The assumption made by the JCVI that the 2 mRNA vaccines, i.e. BNT162b2 (produced by Pfizer & BioNTech) & mRNA-1273 (made by Moderna) would have a similar behaviour to the ChAdOx1 nCOV-2019 Vaccine (produced by the University of Oxford/AstraZeneca) is not supported by published empirical evidence (Folegatti et al., 2020; Widge et al., 2021; Walsh et al., 2020).
Recent findings point out to the importance of quantifying the characteristics and durability of vaccine-induce protection after the 1st dose in order to determine the optimal time interval between the 2 doses (Moghadas et al., 2021). The data from the Phase 1/2 of the ChAdOx1 nCOV-2019 Vaccine (the viral vector DNA vaccine produced by the University of Oxford/AstraZeneca) revealed a substantial specific anti-virus spike protein T-cell response at day 7, which then peaks at day 14 (Folegatti et al., 2020); this response is not seen in the BNT162b2 (the mRNA vaccine produced by Pfizer & BioNTech).
Furthermore, there are marked quantitative differences in the production and duration of neutralising antibodies (NAbs). The two mRNA vaccines i.e. BNT162b2 (produced by Pfizer & BioNTech) & mRNA-1273 (made by Moderna), show marked falls in NAb titres (compared with the Oxford/AstraZeneca viral vector DNA vaccine) in the period before the scheduled second dose [day 22 for BNT162b2 by Pfizer & BioNTech (Mulligan et al., 2020; Collier et al., 2021) & day 29 for mRNA-1273 by Moderna (Widge et al., 2021)], something that has been highlighted as occurring in all age groups. Neutralisation titers are correlated with protection against viral infections post vaccination. It is quite clear that neutralising antibodies (NAbs) titres will continue to fall during days 21-85 [if a 12-week delay is implemented between the 2 doses], leading to very reduced immunity and increased risk to individuals of infection, especially in frail older people. A low efficacy of 52.4% was reported out to day 22 after the 1st dose for BNT162b2 (produced by Pfizer & BioNTech) (Polack et al., 2020), and efficacy of 50-60% has been reported in observational cohort studies from Israel covering the same period (Chodick et al., 2021; Aran, 2021).
Hence, it seems that the UK’s decision for a delayed 2nd dose strategy for the BNT162b2 (produced by Pfizer & BioNTech) is a misguided step; it will provide some protection for patients after a 1st dose, but how much and for how long, is unknown and without patient consent. The main risk is that UK’s 12-week delayed 2nd dose could lead to the emergence of COVID-19 variants resulting from sub-optimal or partial immunity. The Government’s Scientific Advisory Group for Emergencies has also documented concern about emergence of variants as a result of delayed 2nd dose; yet this will not be an issue for the ChAdOx1 nCOV-2019 Vaccine (the viral vector DNA vaccine produced by the University of Oxford/AstraZeneca) but rather for the mRNA vaccines [BNT162b2 (the mRNA vaccine produced by Pfizer & BioNTech) & mRNA-1273 (made by Moderna)]. Sub-optimal vaccination with the 2 mRNA vaccines will lead to selective pressure favouring the emergence of vaccine-resistant variants, which could result in a persisting pandemic. New updated vaccines to target the variants is a possibility, but this will require time for testing, mass production, and distribution; human lives will also be lost.
As already said, in the case of the ChAdOx1 nCOV-2019 Vaccine produced by the University of Oxford/AstraZeneca, the 12-week dosing strategy seems like an excellent decision since that vaccine is different, being a viral vector DNA vaccine, and there is sufficient evidence to back the 12-week gap, but this is not the case for the mRNA based vaccines such as the BNT162b2 Vaccine produced by Pfizer & BioNTech. If escape variants arise due to sub-optimal dosing with BNT162b2, they will likely be resistant to other vaccines that target the same viral spike protein.
To conclude, the 3-week dosing schedule as gold standard (94% efficacy) should be respected for the mRNA based vaccine BNT162b2 produced by Pfizer & BioNTech as supported by the World Health Organisation and adopted by the US Centers for Disease Control and Prevention and there should be no more than a 6-week (42 days) gap between the 2 doses (for exceptional circumstances) as advised by the European Medicines Agency. (Robertson et al., 2021)
A study published in Nature explored the antibody and memory B cell responses of a small cohort of 20 volunteers who received the 2 messenger RNA vaccines Moderna (mRNA-1273) or Pfizer-BioNTech (BNT162b2) and found that 8 weeks after receving their 2nd dose, the plasma neutralising activity and relative number of RBD-specific memory B cells were equivalent to those of individuals who had recovered from natural infection. However, activity against SARS-CoV-2 variants that encode E484K-, N501Y- or K417N/E484K/N501-mutant S was reduced by a small—but significant—margin. Together, these results suggest that the monoclonal antibodies in clinical use should be tested against newly arising variants, and that mRNA vaccines may need to be updated periodically to avoid a potential loss of clinical efficacy (Wang et al., 2021).
Recent research, investigating the neutralisation of viruses with European, South African, and United States SARS-CoV-2 variants with the BNT162b2 mRNA vaccine found that the antibodies elicited by primary infection and by the vaccine are likely to maintain protective efficacy against B.1.1.7 variant (UK) (Muik et al., 2021) and most other variants but the partial resistance of the spike protein found in the B.1.351 (South Africa) variant could lead to some individuals being less well protected (Tada et al., 2021). Further studies showed that the neutralisation of the B.1.351 (South Africa) lineage/variant was robust but lower than the neutralisation of B.1.1.7 (UK) lineage and P.1 (Brazil) lineage (Liu et al., 2021; Xie et al., 2021)
(v) NVX-CoV2373 produced by Novavax
The NVX-CoV2373 produced by Novavax is a protein-based vaccine. Protein subunit vaccines use smaller components of the target pathogen to minimise the risk of unintended allergenic or reactogenic effects [Note: Reactogenicity refers to adverse reactions, especially excessive immunological responses and associated signs and symptoms, including fever and sore arm at the injection site] caused by introducing the whole organism into the host. The protein subunit vaccine used to fight against COVID-19 makes use of the S protein of the SARS-CoV-2 virus as it can trigger the release of neutralizing antibodies and T cells. Similar to killed vaccines, subunit vaccines are not alive and so cannot penetrate host cells. (Loo et al., 2021)
The NVX-CoV2373 vaccine by Novavax uses the coronavirus S protein to generate an antigen using recombinant nanoparticle technology coupled with Novavax’s Matrix-MTM adjuvant to produce their vaccine. Preliminary studies for the vaccine produced promising results whereby it demonstrated high immunogenicity in animal models. High levels of S protein-specific antibodies and SARS-CoV-2 wild-type virus-neutralising bodies were detected after a single immunisation. Upon administering the second dose with adjuvant, the microneutralisation titers further increased 8-fold over responses seen with the first vaccination. As explained above, neutralisation titers are correlated with protection against viral infections post vaccination. Vaccines against viral infections induce protective neutralising antibodies which are markers of protective immunity against reinfections after an initial infection. This suggested that the vaccine would be protective when used in humans.
The NVX-CoV2373 vaccine produced by Novavax has been found to be effective at 95.6% against the original variant of SARS-CoV-2 but also provides protection against newer variants, the UK’s B.1.1.7 variant (85.65% efficacy) and South Africa’s B.1.351 variant (60% efficacy) as preliminary data from clinical trials show. The interim results have been released from a phase III trial carried out in the UK with more than 15,000 participants aged between 18 – 84, including 27% over the age of 65.
The trial tested 2 doses of the vaccine administered 21 days (3 weeks) apart. 62 symptomatic cases of COVID-19 were reported of which 56 were in the placebo group (saline) and 6 in the vaccine group; only 1 case out of the 62 cases of symptomatic COVID-19 was considered as severe and it was in the placebo group, while 32 were in the UK B.1.1.7 variant group of COVID-19. A phase II trial is also ongoing in South Africa with 4400 volunteers, in which 29 cases of COVID-19 have been seen in the placebo group (only 1 severe) and 15 in the vaccine group. Preliminary sequencing data of 27 of these cases found that 93% of them (25) involved the South African COVID-19 variant B.1.351.
Funded in part by the Coalition for Epidemic Preparedness Innovations and the Bill and Melinda Gates Foundation, both the South Africa and UK trial are continuing and further analysis is expected to be shared as more data becomes available. Another phase III trial in the US and Mexico is under way and has randomised more than 16 000 participants; it was expected to hit its 30 000 target by February 2021.
The NVX-CoV2373 vaccine can be stored at 2°C to 8°C and has been found to be safe. An interim analysis of clinical trial data reported that severe, serious, and medically attended adverse events occurred in very low numbers and were balanced between the vaccine and placebo groups. (Mahase, 2021)
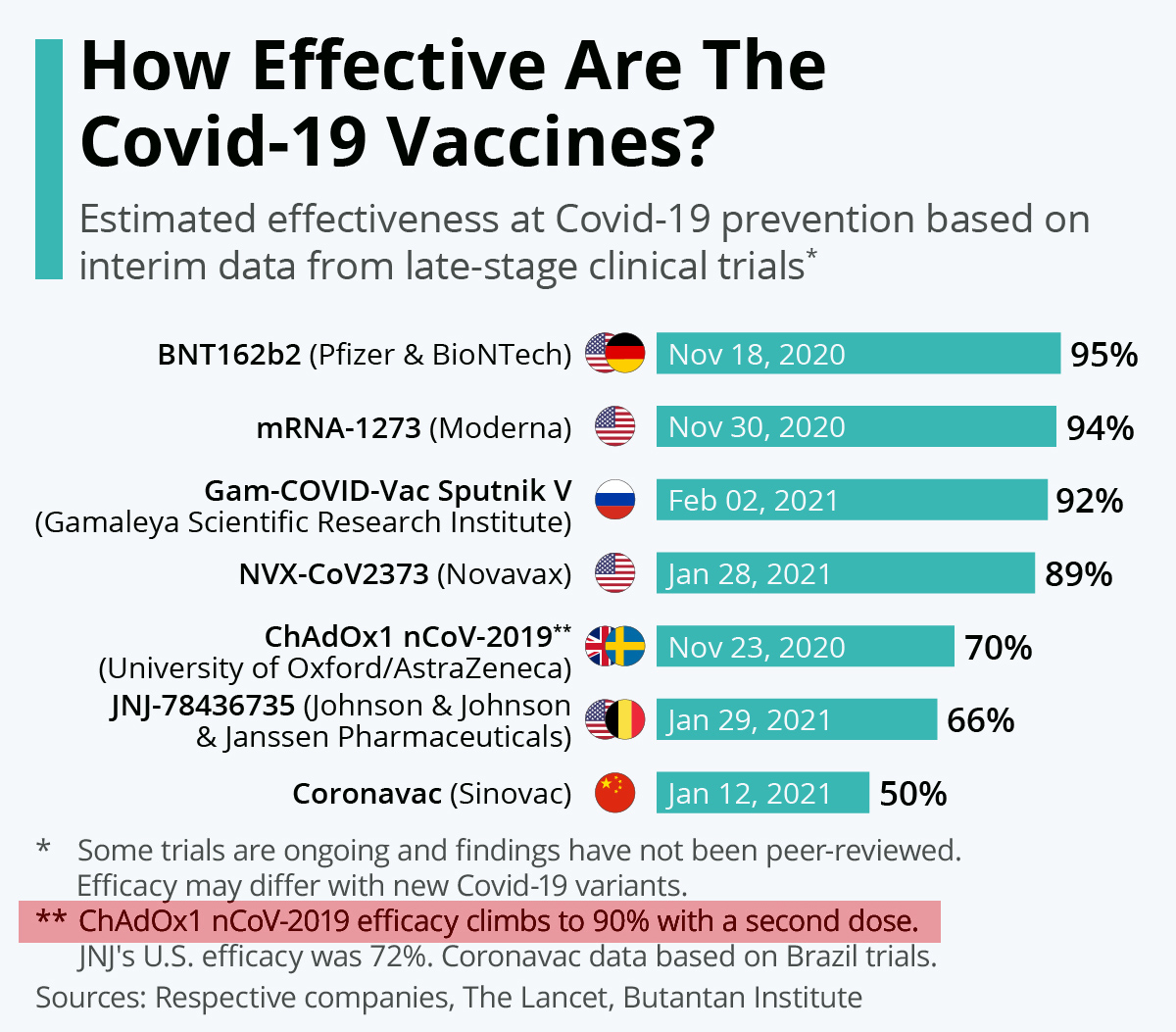
Chart: Quelle est l’efficacité des vaccins Covid-19 ? / How Effective Are The Covid-19 Vaccines? / Source: Statista
(vi) BBV152 Covaxin produced by Bharat Biotech
While Covishield (i.e. the Indian version of Oxford/AstraZeneca’s ChAdOx1 nCOV-2019) uses a weakened version of chimpanzee adenovirus, BBV152 Covaxin uses a human inactivated SARS-CoV-2 virus extracted from an asymptomatic patient. In an inactivated viral vaccine, the target virus has lost the ability to replicate, and it can thus be safely used in a vaccine to trigger an immune response. Inactivated vaccines such as BBV152 Covaxin trigger hymoral responses that release neutralising antibodies. The inactivated viruses cannot penetrate the host cells actively; they can only rely on endocytosis to be taken up into the cells. Inactivated viral vaccines exhibit lesser immunogenicity and have a shorter duration of protection than live vaccine. Therefore, repeat doses or co-administration with an adjuvant or delivery vehicle are needed to overcome weak immune responses after vaccination. The addition of an adjuvant enhances local inflammation by activating the innate immune response, which increases the vaccine’s ability to provoke an adaptive response. (Loo et al., 2021)
In January 2021, the Lancet published the phase I trial data for BBV152 Covaxin, giving it a green light for safety, stating that it generates “adequate” immune response and induced high neutralising antibody responses that remained elevated in all participants 3 months after the second vaccination but said further efficacy trials were needed (Ella et al., 2021). In the phase II trial, the BBV152 Covaxin was given in a 2-dose regimen over 4 weeks (28 days apart) and showed better reactogenicity [Note: Reactogenicity refers to adverse reactions, especially excessive immunological responses and associated signs and symptoms, including fever and sore arm at the injection site] than reported with BNT162b2 and mRNA-1273 and safety outcomes, and was able to induce robust humoral and cell-mediated immune responses compared with phase I trial while no serious adverse events were observed (Ella et al., 2021). The Phase III results of BBV152 Covaxin based on a trial involving 25,800 participants aged between 18 – 98 years old, including 2,433 who were over the age of 60 and 4,500 with comorbidities [the largest ever conducted in India], showed that the vaccine was well tolerated and demonstrated 81% efficacy in preventing COVID-19 in those without prior infection after the 2nd dose. Analysis from the National Institute of Virology also found that the vaccine-induced antibodies can neutralise the UK variant and other heterologous strains.
The BBV152 Covaxin is stable at 2 to 8 degrees celcius and comes in a ready-to-use liquid formulation. Clinical trial is ongoing to the final analysis at 130 confirmed cases in order to gather further data and evaluate the BBV152 Covaxin in additional secondary study endpoints.
A hurried approval of India’s own BBV152 Covaxin, manufactured by Bharat Biotech in collaboration with the Indian Council of Medical Research and National Institute of Virology has undermined public trust among its own citizens. Activists in India are mainly criticising the way in which BBV152 Covaxin’s phase III clinical trials have been conducted. 700 people were recruited by the People’s University, a privately run medical college and hospital, who paid 750 Indian Rupees (£ 7.50; 8 Euros; $ 10.30) to each. However, there are no records of informed consent, despite audiovisual recording of consent from people who cannot read or write being mandatory since 2013. Hence, many participants did not understand they were taking part in a trial and thought the jab was simply COVID-19 protection, while the follow-up was also inadequate since they could not describe their reactions in written form adequately, many family members share one phone and not every participant was available for such monitoring. Hence, the major confusion arose due to the lack of transparency. Anant Bhan, an adjunct professor at Yenepoya University pointed out: “As the number of participants in a trial increases, there’s a higher chance you will catch adverse events, which would be relatively rarer in smaller groups,” he says. “This is why efficacy data is important to know—safety is an ongoing process even in phase 4, as you market the vaccine.“, adding “It’s concerning, because all this could have an impact on public trust in the vaccine, undermining such a critical public health intervention.”
As already mentioned, Covishield is the better known out of the 2 vaccines produced in India, it is an Indian version of the Oxford University-AstraZeneca vaccine made by the world’s largest vaccines manufacturer, the Serum Institute of India, and we know that in India, people feel safer with the Covishield vaccine instead of India’s own BBV152 Covaxin. This has been confirmed in a nationwide survey in India among undergraduate medical students through an online questionnaire completed by 1068 medical students across 22 states. Choosing between the well-known Covishield (developed by Oxford-AstraZeneca) and India’s BBV152 Covaxin was considered as important by medical students both for themselves and their future patients, where Covishield was preferred to Covaxin (Jain et al., 2021).
A survey has also been conducted in India regarding the adverse effects and symptoms following COVID-19 vaccination where 5396 people responded. Among those who responded the majority were doctors (85.8%), followed by nurses (6.2%), technicians (1.1%) and others. 56% of the respondents were male and 44% female.
Among the respondents, 5128 (95%) received Covishield (which the Oxford-AstraZeneca vaccine manufactured by Serum Institute in India), 180 (3.3 %) received BBV152 Covaxin (manufactured by Bharat Biotech in India), while 44 (0.8%) had received Pfizer-BioNTech and Sinopharm vaccines from other nations.

Chart showing type of vaccine received by the 5396 respondents. (Jayadevan et al., 2021)
Overall, 65.9% of respondents reported experiencing at least one post-vaccination symptom such as:
Tiredness (45%), myalgia (44%), fever (34%), headache (28%), local pain at injection site (27%), joint pain (12%), nausea (8%) and diarrhoea (3%) were the most prevalent symptoms. All other symptoms were 1% or less (See the chart below).

Chart showing post-vaccination symptoms among 5396 respondents. (Jayadevan et al., 2021)
To conclude, two-thirds of healthcare professionals who completed the survey reported mild and short-lived post-vaccination symptoms. Tiredness, myalgia and fever were most commonly reported. These symptoms were consistent with an immune response commonly associated with vaccines, and correlated with the findings from previously published phase 2/3 trials.
In 90% of the cases, the symptoms were either milder than expected or meeting the expectation of the vaccine recipient. No serious events were reported. Symptoms were more common among younger individuals and there was no difference in symptoms among those who had a past history of COVID-19 (Jayadevan et al., 2021).
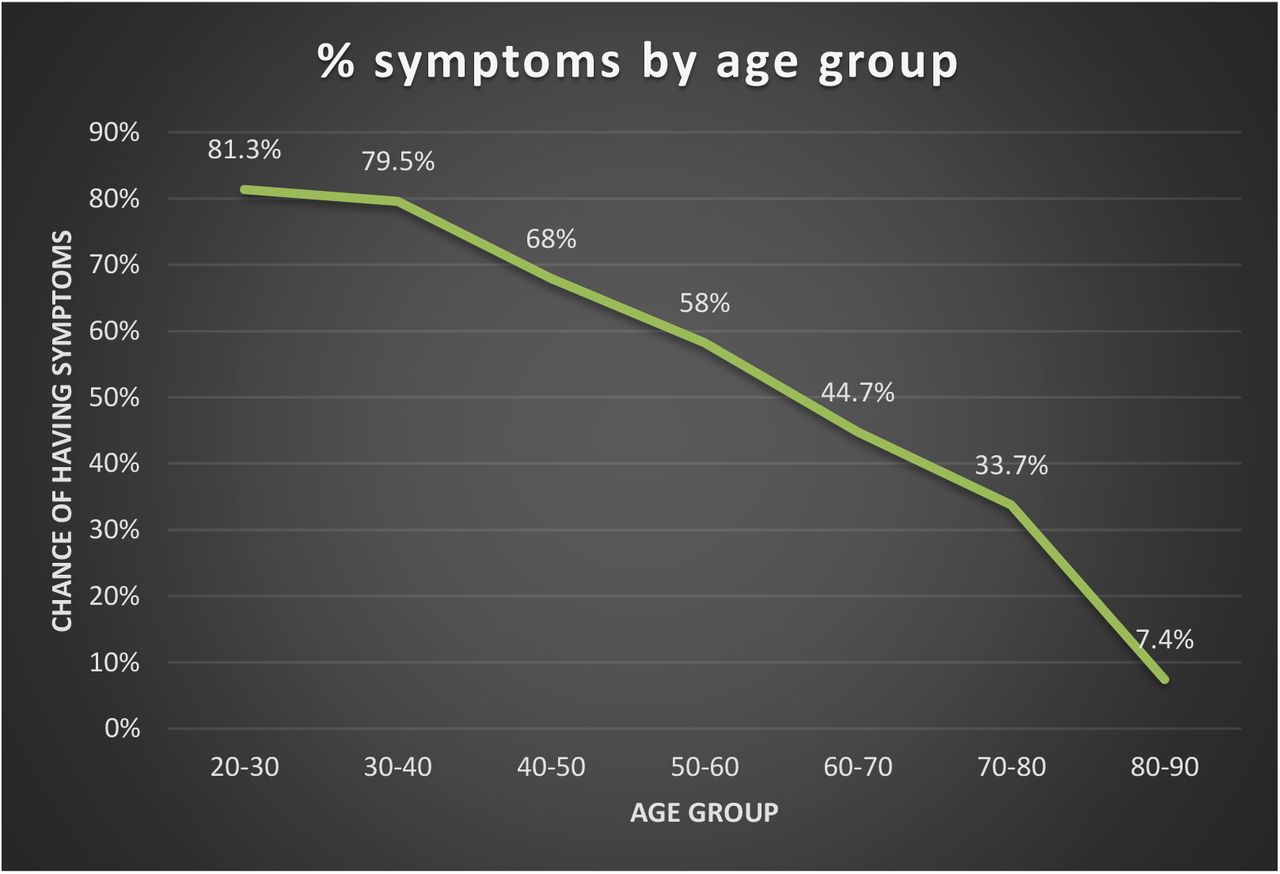
Chart showing % chance of experiencing adverse symptoms of post-vaccination among 5396 respondents by age group (Jayadevan et al., 2021)
There are also a range of other vaccines worldwide, however those 6 vaccines presented and discussed above are the most popular ones with data and real world deployment to support their efficacy.
The first COVID-19 vaccine to be approved in the western world, BNT162b2 (Pfizer), was closely followed by mRNA-1273 (Moderna), and the chimpanzee-adenovirus vectored AZD1222 (AstraZeneca–Oxford). Unfortunately, cold-chain requirements, finite global manufacturing capacity, and insufficient supply are likely to disproportinately affect low-income and middle-income countries (LMICs). Mathematical models indicate that there will not be an adequate supply of vaccines available to cover the global population until 2023, further exacerbating health and other disparities in LMICs.
India’s own vaccine, BBV152 Covaxin, produced by Bharat Biotech, is a welcome addition since the company is experienced in the development of a wide range of vaccines [influenza H1N1, Rotavirus, Japanese Encephalitis, Rabies, Chikungunya, Zika and the world’s first tetanus-toxoid conjugated vaccine for Typhoid] and distribution to low-income and middle-income countries (LMICs), and is poised to bridge vaccine disparity gap using its BBV152 Covaxin which has an almost similar efficacy to the Oxford/AstraZeneca’s ChAdOx1 nCOV-2019 [81% efficacy from Phase III clinical trials] hence slightly inferior compared to the 2 mRNA vaccines, BNT162b21 [94% efficacy] and mRNA-1273 [94.5% efficacy], the NVX-CoV2373 vaccine [95.6% efficacy] and the Gam-COVID-Vac Sputnik V Vaccine [91.6% efficacy]. However, while vaccinated people may still become infected with COVID-19, all those vaccines should prevent severe and life-threatening symptoms.
In India, Covishield (i.e. the Indian version of Oxford/AstraZeneca’s ChAdOx1 nCOV-2019) & BBV152 Covaxin are being provided for free to frontline workers, with no choice as to which one a recipient receive. Both vaccines require the usual two doses and work by priming the immune system with a SARS-CoV-2 spike protein. The vaccines are paid for by the Indian government, who declared that the 2 vaccines cost them a quarter of the price on the global market, making them the cheapest in the world. The Oxford-AstraZeneca Covishield is priced at £ 2.01 (200 Indian Rupees) and Bharat Biotech’s BBV152 Covaxin will cost £ 2.97 (295 Indian Rupees) for a single dose. However, when India’s vaccines reach the private market, those prices are expected to be much higher. Covishield is expected to increase by 5 times, reaching around £ 10.05 (1000 Indian Rupees) per dose and at this moment there are no measure in place to keep them affordable for those who desperately need it. With the world’s second largest population, at 1.36 billion, there is a huge potential market in India where more than 160 000 COVID-19 deaths have so far been recorded while also being the country with the second highest number of infections worldwide; it also has one of the largest pharmaceutical manufacturing capacities in the world, so the Asian country seems well placed to deal as both importer and exporter, and has a central role to play in the planetary immunisation efforts against the COVID-19 pandemic.
In December 2020, the US pharmaceutical company Ocugen signed a letter of intent to codevelop Bharat Biotech’s vaccine, BBV152 Covaxin, for the American market. And in the wake of mixed efficacy results for the Chinese Sinovac, Brazil has also looked to India for both BBV152 Covaxin and Covishield stocks. By 23 January 2021, 2 million doses of Covishield had already been delivered to Brazil, while a memorandum has been signed by private Brazilian clinics for 5 million doses of BBV152 Covaxin to be delivered by March 2021.
Biotech companies in India are also expected to produce 300 million doses of Russia’s Sputnik V vaccine. This may come as crucial since the powdered version of the Sputnik V vaccine can be stored at refrigerator temperatures, making it more suitable for warmer climates. Novavax is also expected to have 2 billion doses of its NVX-CoV2371 produced per year by the Serum Institute of India. All this puts India in a prime position to both benefit from the world’s vaccine need and provide for its own gigantic population.
Pfizer and Oxford-AstraZeneca are reported to be in discussions regarding updating their vaccines to target new variants. The Oxford AstraZeneca team announced that the updated vaccine could be available by autumn 2021. It is possible it could take the form of a one dose booster which is updated and rolled out every year.
Maintaining vigilance after vaccination
It is also important to note that being vaccinated is not a guarantee of instant and/or absolute protection. Like all medicines, no vaccine is completely effective, so individuals should continue to take precautions to avoid infection. Some people may still be infected with COVID-19 despite being vaccinated, however their symptoms should be less severe and not life-threatening once the vaccine’s immunity has fully developped after the completed 2 doses with the perfectly timed interval [depending on the vaccine type].
Vaccines do not provide instant immunity; people have little or no immunity at all to the coronavirus immediately after their first jab. Full immunity can take as long as 3 weeks to develop!
Experts have called for stronger health warnings for people vaccinated against COVID-19 after observing a rise in infections shortly after vaccination, suggesting that many people are unaware of the danger and are letting their guard down before the vaccine has taken effect.
A study conducted by Public Health England in the over 70s found a “notable” rise in COVID-19 infections in people immediately after they received the AstraZeneca vaccine (Bernal et al., 2021). Similary another study on Israel’s vaccination programme, found a similar spike in cases among people who had just been jabbed; it was observed that the daily incidence approximately doubled after vaccination until about day 8 (Hunter and Brainard, 2021). A survey conducted in the UK by the Office for National Statistics, investigating COVID-19 and vaccine attitudes and behaviours in England, explains why those spikes may be taking place. Among over 80s who had received their 1st dose of vaccine in the previous 3 weeks, a staggering 41% reported having met up with someone other than a household member, care worker, or member of their support bubble indoors since vaccination, thereby breaking lockdown regulations.
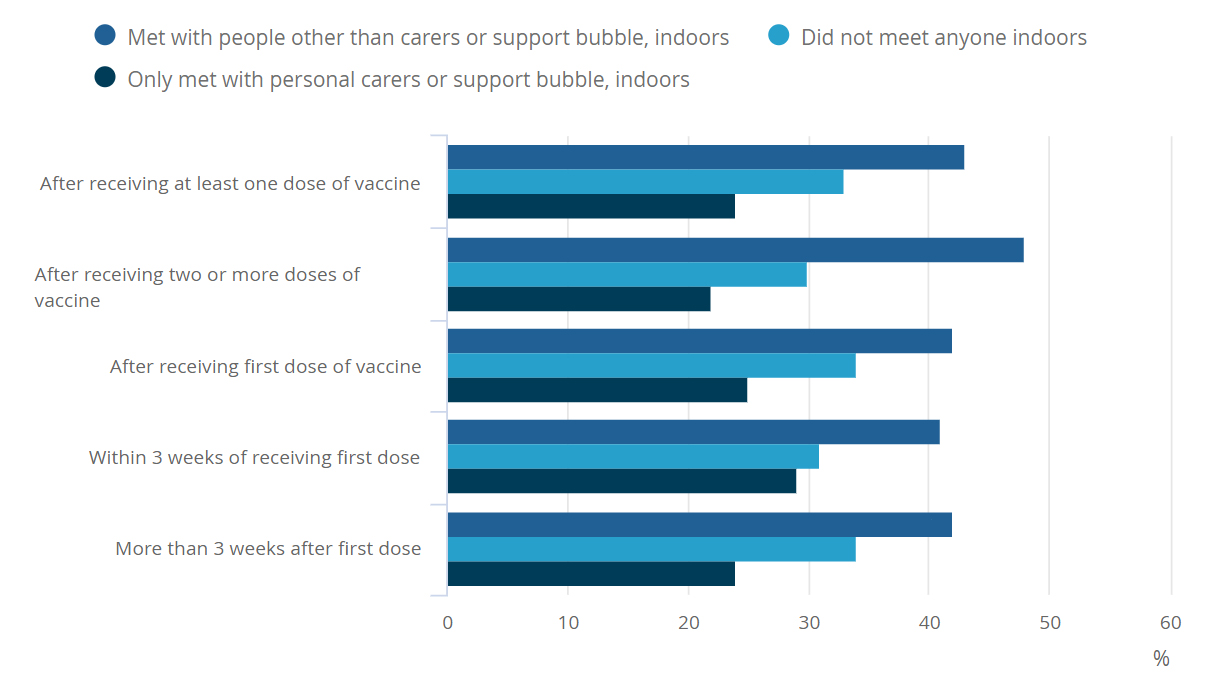
Percentage of over 80s, by who they had met indoors, since being vaccinated against COVID-19, by how many doses of vaccine they have received, England, 15 February to 20 February 2021 / Source: ONS

Percentage of all over 80s, by how much they perceived the coronavirus (COVID-19) to be a risk to them personally, after hypothetically receiving each dose of vaccine, England, 15 February to 20 February 2021 / Source: ONS
Hence, a group of health psychologists from King’s College, London, University College London and the University of East Anglia have written in the British Medical Journal that the studies, considered together, suggest that there is an urgent need to ramp up health warnings. “Looking at both strands of research—from Israel and the UK—it’s reasonable to suggest people are letting their guard down after they have their first dose,” said James Rubin, professor of psychology of emerging health risks at King’s. “The research has shown that immediately after a first jab people are more likely to be flouting social distancing, meeting people outside their household or bubble—and meeting them indoors.”
A YouGov survey conducted in December 2020 revealed that 29% of people would follow pandemic related rules and restrictions less strictly once they were vaccinated. Paul Hunter, professor of health protection at the University of East Anglia, who reviewed the Israeli data, drew similar conclusions. “While it is not possible to know for certain why this [the spike in cases soon after vaccination] may be the case, there have been concerns that people may believe they are protected as soon as they have had . . . their first injection and so start engaging in risky behaviour more than previously,” he said.
James Rubin said that authorities needed to ram home the message that people have little or no immunity to the coronavirus immediately after their first jab. Full immunity can take as long as three weeks to develop. This message must be clarified and made very clear to publics worldwide. The British Medical Journal asked Public Health England to comment on the suggestion that health leaflets should give greater emphasis to the fact that vaccines do not provide immediate immunity. Rubin said that the NHS should also consider hammering home the message verbally. He said, “I do think that this one-to-one situation, when the person is getting jabbed, is a perfect opportunity for the person giving the vaccine to say that the recipient won’t be protected for a few weeks—and to remind them that they need to continue sticking to the rules on social distancing and not meeting people outside their household or bubbles.”
Vaccines must be monitored for future side-effects & the safest vaccine selected
The rapid increase in morbidity and mortality of the COVID-19 pandemic has led to a drastic shift in the conventional vaccine development paradigm and timelines from a time frame of 10–15 years to 1–2 years (Lurie, Saville, Hatchett and Halton, 2020). The change in the development time frame could mean researchers cannot ascertain the vaccine-induced protective immunity’s longevity and quality. In an ideal world, a vaccine should have high efficacy, with minimum adverse reactions. It should stimulate both humoral and cell-mediated immune responses while being able to induce life-long immunity in the recipients.
It is important to understand that different vaccine platforms’ have been deeply studied and each one has its benefits and limitations [as the table above shows].
In order to overcome the limitations of particular vacccine platforms [technology] a range of techniques have been developed to modify the vaccine platforms to ensure the safety and efficacy of the vaccines before they are distributed and administered. In the case of inactivated viral vaccines [such as BBV152 Covaxin] and protein subunit vaccines [such as NVX-CoV2373 vaccine by Novavax], the antigens in the vaccine by itself may have inadequate immunostimulatory capabilities, hence to compensate for this weakness, additional adjuvants have to be added. Adjuvants generally trigger the innate immune response to recognise the components of the vaccine as a threat to the host [patient’s body], leading to the activation of the antigen-presenting cells, resulting in adaptive immune activities (Coffman, Sher and Seder, 2010). This leads to an increased vaccinal efficacy and extends the duration of the vaccine; it could also lead to a lower dosing frequency to achieve immunity towards the pathogen. However, one of the side effects of adjuvants is that it may increase reactions such as pain, redness, and swelling at the injection site and a few other symptoms such as fever, fatigue, and myalgia (Garçon, Segal, Tavares and Van Mechelen, 2011) due to enhanced activation of the immune response, resulting in inflammation at the injection site.
Currently, the 2 mRNA vaccines developed by Pfizer and Moderna do not use adjuvants. Prime-boost techniques have also been utilised to develop higher immunity levels compared to immune responses obtained by a single vaccination. This method aims to induce both humoral and cellular immune responses to provide long-lasting immunity. An example would be the use of a heterologous prime-boost method involving a viral vector for priming a protein-based vaccine as the booster, which allows for the induction of a strong cellular immune response and a higher specificity of antibodies produced against the target of the vaccine.
Studies have shown that the modifications made to vaccines could lead to other side effects even though they may increase the vaccine’s effectiveness. There have been instances in the past where licensed vaccines have been withdrawn from the market due to newly discovered adverse events associated with them. Hence, a strict assessment of the benefit-to-risk ratio is vital to ensure that the continued use of a particular vaccine provides more benefits than harm to the public.
As the COVID-19 pandemic comes under control or new information regarding the vaccine surfaces, assessments of the benefits of the vaccines may change. Hence, health authorities should assess which vaccine will be the most suitable and effective in our planetary fight against the COVID-19 pandemic. Each vaccine has demonstrated that it can elicit an immune response and has a relatively good safety profile even if all the vaccine platforms used have advantages and disadvantages.
The choice of the best and ultimate vaccine ultimately depends on the knowledge of the pathophysiology of SARS-CoV-2 [i.e. the COVID-19 virus] and the exact immune response required for protection. The ultimate vaccine should be confirmed as one that can be used without severe complications in the patient post immunisation. Relentless monitoring of recipients of the vaccine is essential to detect any severe adverse reactions to ensure the vaccine is safe for the long term health of future generations.
A good and reliable vaccine must be easily administered and remain stable during transport and storage [one of the disadvantages of the 2 mRNA COVID-19 baccines is the extreme low temperature storage requirement]. From an economic standpoint, the manufacturing process of a good vaccine should be reproducible and inexpensive to be easily translated to developing countries. Once an effective vaccine is developed, it is crucial that there is equitable access and distribution of vaccines across all nations to protect the public’s health. Demographics at a higher risk should also be prioritised in receiving the vaccine to prevent further spread and fatalities, because no country will be safe until the whole world is.
Understanding the importance of strategy for successful vaccination campaigns
Vaccination campaigns to control the COVID-19 pandemic on the planet is not simply dependent on the vaccine efficacy and safety. The acceptance of the vaccine among the publics worldwide and healthcare workers has a decisive role in the successful immunisation of the human population and the control of this pandemic. A systematic review has been conducted in order to provide an assessment of COVID-19 vaccination acceptance rates worldwide. The results from 31 peer-reviewed published studies met the inclusion criteria and formed the basis for the final COVID-19 vaccine acceptance estimates rates, found from 33 different countries. Among adults representing the general public, the highest COVID-19 vaccine acceptance rates were found in Ecuador (97.0%), Malaysia (94.3%), Indonesia (93.3%) and China (91.3%). However, the lowest COVID-19 vaccine acceptance rates were found in Kuwait (23.6%), Jordan (28.4%), Italy (53.7), Russia (54.9%), Poland (56.3%), US (56.9%), and France (58.9%). Only eight surveys among healthcare workers (doctors and nurses) were found, with vaccine acceptance rates ranging from 27.7% in the Democratic Republic of the Congo to 78.1% in Israel. In the majority of survey studies among the general public stratified per country (29/47, 62%), the acceptance of COVID-19 vaccination showed a level of ≥70%. Low rates of COVID-19 vaccine acceptance were reported in the Middle East, Russia, Africa and several European countries.
This could represent a major problem in the global efforts to control the current COVID-19 pandemic. More studies are recommended to address the scope of COVID-19 vaccine hesitancy. Such studies are particularly needed in the Middle East and North Africa, Sub-Saharan Africa, Eastern Europe, Central Asia, Middle and South America. Addressing the scope of COVID-19 vaccine hesitancy in various countries is recommended as an initial step for building trust in COVID-19 vaccination efforts (Sallam, 2021).
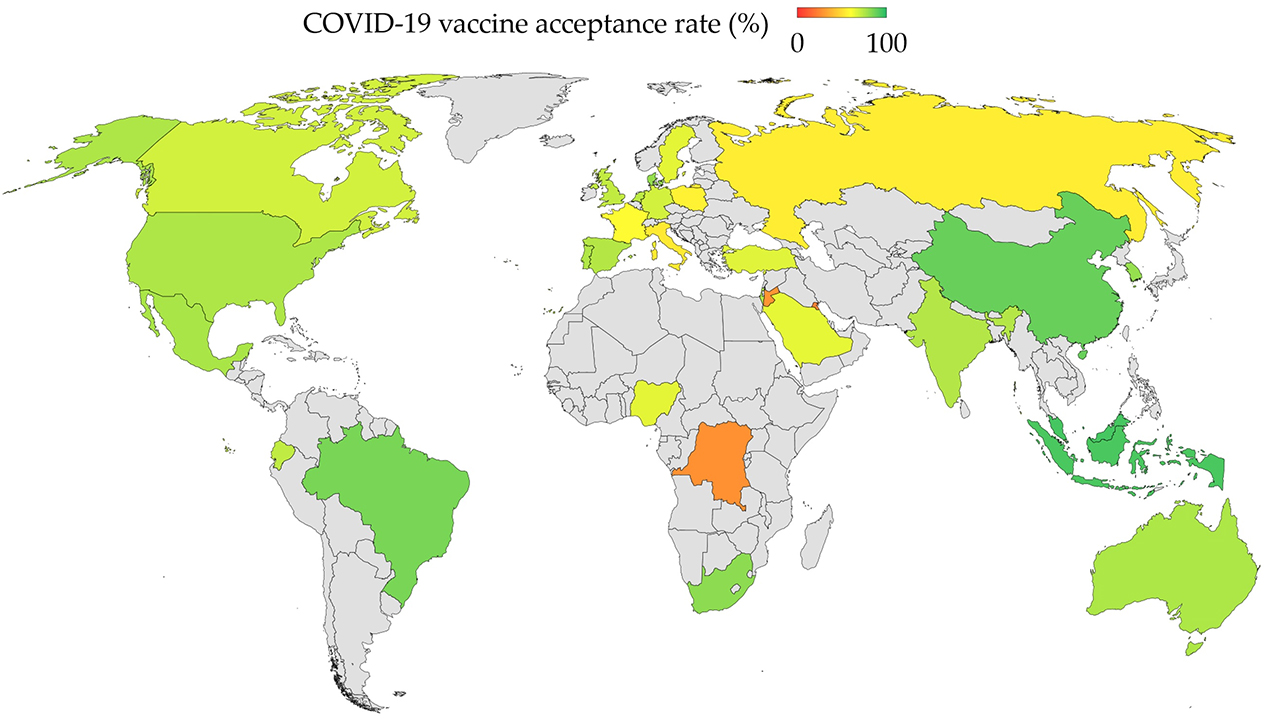
Map: COVID-19 vaccine acceptance rates worldwide (Sallam, 2021)
In order to encourage people to get vaccinated, one of the most important persuasive factor remains the safety of the vaccine. A study conducted found that people who perceive COVID-19 as a severe disease were more intent on taking a COVID-19 vaccine. Hence, informing publics worldwide about the safety of the COVID-19 vaccine(s) should be the focus for health authorities aiming to achieve a high vaccine uptake in the course to immunise the human population on the planet (Karlsson et al., 2021). In the UK 4 in 5 adults (86%) who were reluctant or intending to refuse a COVID-19 vaccine in December 2020 had changed their mind by February 2021 and planned on getting vaccinated or had already been vaccinated, as a UCL cohort study on trends, patterns and psychological influences on COVID-19 vaccination intention shows.
In the Middle East, 3 countries, Israel, the United Arab Emirates (UAE), and Bahrain, have successfully administered the vaccine to a high percentage of their populations compared to the rest of the world. These Middle Eastern states have put continuous effort into reassuring the public that the vaccine is safe and effective. Through its universal healthcare system, within days, Israel vaccinated almost 11.0 doses per 100 population and the next highest rate was 3.5 in Bahrain. The vaccination in these countries was higher compared to that in the United Kingdom, the United States of America, and even China (Rosen, Waitzberg and Israeli, 2021).
Another study confirmed that factors related to the implementation will contribute more to the success of vaccination programs than a vaccine’s efficacy itself. The benefits of a vaccine will decline substantially if we face manufacturing or deployment delays, significant vaccine hesitancy or greater epidemic severity.
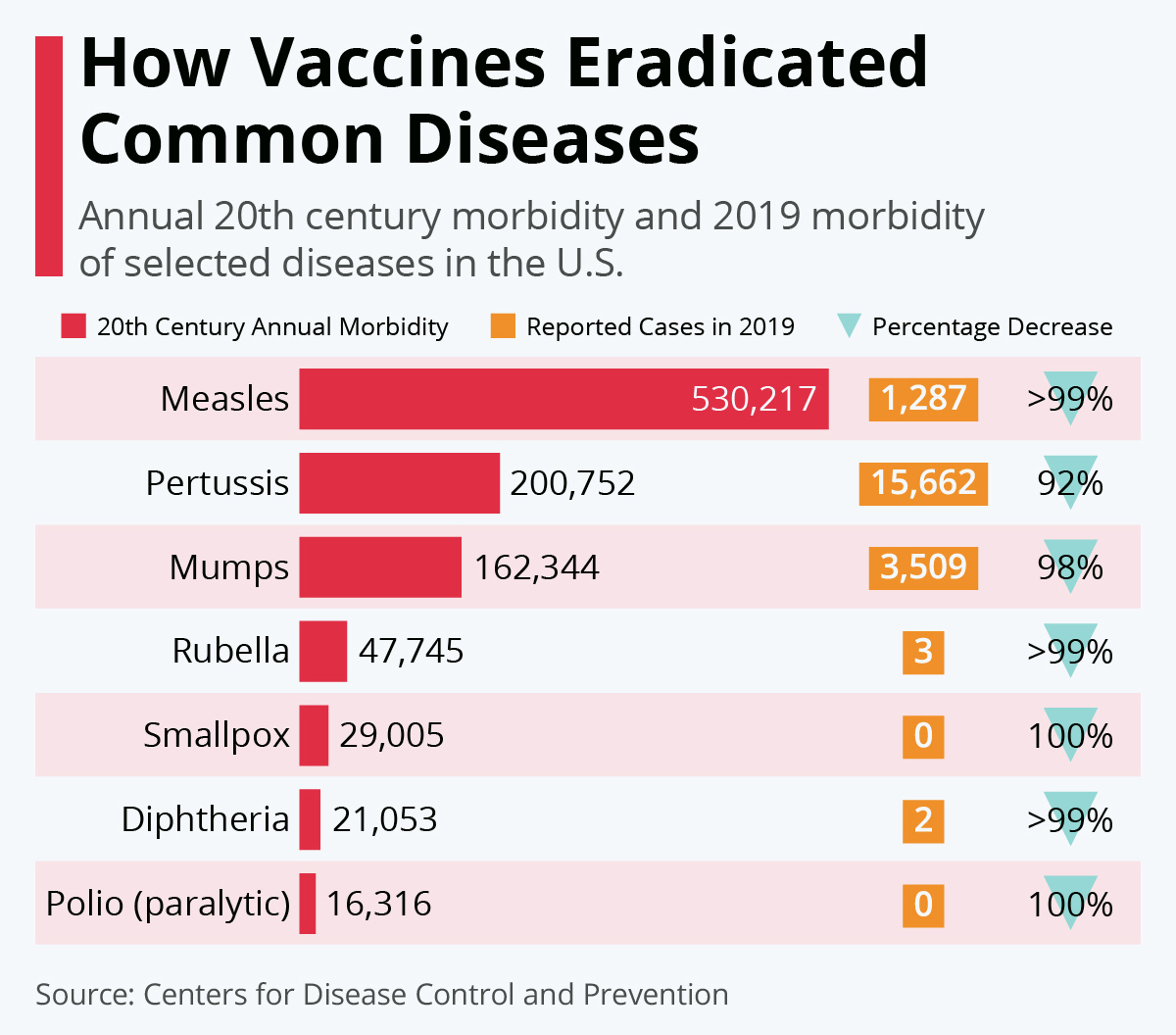
Chart: Comment les vaccins ont éradiqué des maladies courantes / How Vaccines Eradicated Common Diseases Source: Statista
Hence, it is fundamental for health authorities and officials to invest greater financial resources and attention to vaccine production and distribution programs, to redouble efforts to promote public confidence in COVID-19 vaccines and to encourage continued adherence to other mitigation approaches (Paltiel et al., 2021).
The planetary urgency for equitable distribution of COVID-19 vaccines and treatments
COVAX, launched in April 2020 is an initiative led by 3 global organisations [GAVI, CEPI & The World Health Organisation] that supports the research, development, manufacturing, and price negotiation of the COVID-19 vaccines. COVAX has been established to accelerate the successful development of a vaccine for COVID-19 and initiatives have been implemented to ensure that nations with lower incomes will also be able to receive the vaccines.
However, reports have surfaced that the larger industrial economies, countries such as Canada, the US and the UK have purchased enough doses of vaccines to vaccinate their population multiple times over (Dogra et al., 2021). It is important to note that as the big industrial economies place excessive vaccine orders, the ability of other countries to procure COVID-19 vaccines could be severely undermined and could lead to more deaths and continued contamination globally from various types of travel – no country is safe until the whole human population is immunised against COVID-19. Wealthier countries with only 14% of the world’s population have purchased 53% of the 8 most promising vaccines, the People’s Vaccine Alliance said, this includes all of the doses of the mRNA-1273 vaccine [made by Moderna] to be produced over 2021 and 96% of the BNT162b2 vaccine [made by Pfizer & BioNTech] doses. When the pandemic is ravaging mankind across the planet, this voracious and unnecessary hoarding of vaccines is simply the kind of scenario that could have only been triggered by the collective neuronal activity of irrational imbeciles.
The People’s Vaccine Alliance, that has gained strong support among a wide range of public figures worldwide declared that AstraZeneca-Oxford, Moderna, Pfizer-BioNTech had received more than 5 billion USD of public funding in the development of their vaccines. Significant supply deals have been struck with national governments for those 8 vaccines: Pfizer-BioNTech, Moderna, AstraZeneca-Oxford, Novavax, Johnson & Johnson, Sanofi-GSK, Gamaleya-Sputnik, and Sinovac. While on the other side, some 67 low income countries have made no purchases on their own and are completely dependent on the World Health Organisation’s COVAX programme – a collaboration involving WHO, UNICEF, the World Bank, and the Bill & Melinda Gates Foundation, among others. That programme has managed to secured only about 700 million doses, which is just enough to immunise about 10% of the population in 67 low-income countries.
As a goodwill diplomatic gesture, the Asian vaccine-manufacturing giant, India, is donating 800,000 doses of Covishield. In the same noble path, Oxford University and AstraZeneca have pledged to distribute 64% of their ChAdOx1 nCOV-2019 Vaccine in developing nations, yet, this will only reach 18% of the world’s population in 2021, the Alliance said. The world’s population count is around 8 billion, for those who are not specifically gifted with numbers, this means 8000 million [8000 000 000], and it is on the rise with predictions pointing to almost 10 billion by 2050.

Densité de la population mondiale / World Population Density (personnes/km2) (Source: Worldometer)
A spokesman for Health Canada upon being querried about the excessive vaccine orders, noted that the country had invested £262 million in the COVAX initiative, most of which would be used towards the vaccinal needs of other countries. Experts believe that rich countries will eventually donate their unneeded stocks of vaccines directly to COVAX, but that was not how the programme was supposed to work. However, those countries will first wait to find out about each vaccine’s performance and durability, and the likely consequence will be that we will not be able to reach complete human immunisation on the planet as citizens of poor countries will not be vaccinated until 2022 or 2023.
The People’s Vaccine Alliance have declared that at least 90% of the population in 67 low income countries stand little chance of getting vaccinated against COVID-19 in 2021 because wealthy nations have reserved more than what they require. Selfish and greedy vaccine developers are also refusing to share their intellectual property [which is the vaccine technology used], making it impossible for the vaccines to be produced elsewhere. If the situation remains static, billions of people all over the planet may not be vaccinated for years to come, Oxfam’s health policy manager, Anna Marriott observed. Wealthier nations have enough doses of COVID-19 vaccines to jab their populations almost 3 times over, whilst poor countries do not even have enough to reach health workers and people at risk.
The current system where pharmaceutical corporations use government funding for research, and then retain exclusive rights whilst also keeping their technology secret to boost their profits could cost many lives. Pharmaceutical companies like any other business need financial revenue to cover their costs and develop vaccines and treatments, and in normal circumstances, most people do not have anything against buying their multi-vitamins, toothpastes, mouthwash, pain-relieving pills, pet shampoo or flea-repellent and other drugs at a pharmacie (drug store). However, we are facing a historical pandemic and most of the research and development (R&D) costs to finding a vaccine were financed by public money, hence many humanitarian organisations find it unscrupulous for pharmaceutical giants to charge exorbitant amounts as is the case for other medicines. Pfizer, is selling its COVID-19 BNT162b2 Vaccine for around 39 USD for 2 doses, this works out at an 80% profit margin and puts it beyond the reach of all but the wealthier countries.
Pharmaceutical corporations and research institutions working on COVID-19 vaccines must act with dignity in this global humanitarian crisis; vaccines are not as straightforward as many other medicines to copy since many are composed of very specific biological material. The People’s Vaccine movement argue that since most of the treatments and vaccines have been funded by taxpayer money, governments should impose conditions on their pricing and request corporations and research institutions to share the science, technological know-how, and intellectual property related to the vaccines to maximise production by other quality producers across the planet. Besides, we already have a global mechanism that facilitates this sharing, which is the World Health Organization COVID-19 Technology Access Pool (C-TAP). This would allow enough safe and effective doses to be supplied at a faster rate to all those who also urgently need them; it would also speed up our planetary goal of immunising the world’s population. In the past, the creation of the Medicine Patent Pool for HIV medication resulted in the production of millions of affordable doses of antiretroviral drugs that are today accessible and still being used to save lives in developing countries; this is something that should inspire contribution to the C-TAP (COVID-19 Technology Access Pool).
In those times of crisis, the world’s governments should be focusing on waging a war against death by maximising vaccine production and supplies instead of maximising profits for pharmaceutical giants. For example, Oxford University & Astra Zeneca have licensed production of their ChAdOx1 nCOV-2019 Vaccine to companies in India, Brazil and in Argentina, other vaccine developers should take notice and follow a similar path. The University of Oxford and Vaccitech, having joint rights in the vaccine, entered into a partnership with AstraZeneca in April 2020 for further development, large-scale manufacture and global supply of the vaccine. Equitable access to the vaccine is a key component of the partnership. Neither Oxford University nor Vaccitech will receive any royalties during the pandemic period or from any sales of the vaccine in developing countries.
Vaccine development has progressed impressively fast, however the efforts to provide access to vaccination globally are disgustingly slow. A proposal has been made by South Africa and India to the World Trade Organisation to waive intellectual property rights on COVID-19 vaccines, tests and treatments until the whole human population is protected from COVID-19. Hence, this is an initiative that governments worldwide must support and do everything that is required to ensure that quality COVID-19 vaccines and treatments are made a global public good, freely accessible and distributed simultaneously and quickly across the planet to all its inhabitants in order to eradicate COVID-19 as fast as possible and focus on putting civilisation back on track.
The People’s Vaccine Alliance argued that if COVAX is considering a tiered pricing model, many low and middle-income countries, already faced with economic instability and with under-resourced health systems, will not be able to afford the vaccine or would have to do so at the expense of being even more indebted. COVAX will only succeed if they speed up and maximise production of vaccines by pressuring phamaceutical companies and research institutions to share the science, technology and know-how behind the vaccines with the World Health Organization COVID-19 Technology Access Pool (C-TAP), secure low and transparent vaccine prices and ensure equitable distribution according to the WHO’s equitable allocation framework.

Nombre total de doses de vaccins contre le COVID-19 produit par pays / Total number of doses of COVID-19 vaccine produced per country (Source: Statista France)
The People’s Vaccine Alliance declared that donors should contribute towards vaccine purchases through the global mechanism COVAX.
COVAX should strongly consider the fact that governments have funded much of the research and development costs of vaccines and treatments when they are negotiating the prices. The governments of lower and middle-income countries must also increase and prioritise financing for health services so that vaccines can be acquired as soon as they are available. We are facing a global pandemic with intolerable economic costs for all nations, but this is even worse for the poorest nations. Vaccines, tests and treatments should be supplied at transparent affordable prices so that donors, governments and other charitable associations can afford enough for everyone and provide them free of charge to everyone. Using the HIV treatment as an example, when the price was high people in developing countries were denied life-saving treatment, which resulted in millions of needless death. This changed when generic competition forced the prices down, allowing donors to buy millions of treatments with over 20 million people today benefiting.
The fundamental urgency is to scale up vaccine production across the planet; every manufacturer with the possibility to produce vaccines should be doing so, since it seems barbaric and embarrassing for wealthier nations to be openly vying with each other to secure exclusive access to vaccines while the majority of the human population are left in the cold to watch and wonder about their fate.

Image: Des politiciens dans une démonstration d’agression primitive / Politicians in a display of primitive aggression [Plus d’informations ici / More here: Essay // Psychology: Causes of Aggressive Behaviour in Human Primates]
The People’s Vaccine Alliance believe in an equitable system for prioritising access to those most at risk across the globe, i.e. health and care workers, senior citizens above the age of 60 and all those with chronic conditions – vaccine distribution should be distributed according to necessity rather than being auctioned to the highest bidder. COVAX is currently the only global mechanism for pooling demand for COVID-19 vaccines for lower-income countries and it is encouraging to see that 194 countries have agreed to work together, but the larger industrial economies continue to cut bilateral supply deals with pharmaceutical companies, hence undermining a synchronised worldwide effort towards a systematic and simultaneous vaccine distribution based on an equitable system of distribution to cover the globe.
It is fundamental for everyone on this small over-populated and depleting blue planet to understand no country will truly be safe until all countries are. This is not simply a catch phrase to play good samaritan, but to sensible thinkers it is simply insightful reasoning; because we are not living in the 1950s anymore, the world, its inhabitants, mentalities and human culture has drastically changed. Nowadays, with the post-modern economic development of the 21st century, standards of living have risen worldwide and with the competition in the transportation industries, air tickets have become more affordable; that simply brings forward the fact that no one on Earth is far from one another, since it only takes an address, a phone number, about 20 hours of flight, few hours of driving and a phone call to meet anyone, anywhere & anytime on this small planet.

Image: Décollage d’un avion / Plane taking off
The world is more interconnected as it never was before and this means that if the human population is not immunised as fast as possible, this deadly COVID-19 virus will continue to circulate and be passed around across borders from the wide range of interactions, transactions and exchanges that take place across the planet.
Many groups worldwide are advocating for a people’s vaccine [#PeoplesVaccine] and not a profit vaccine since the COVID-19 is an alarming planetary situation – probably the major pandemic that will be studied and remembered in the centuries to come as part of the history of the 21st century; the campaign is gaining momentum worldwide. Researchers are hopeful that once a greater percentage of the general population receives the vaccine, herd immunity across the planet can be achieved, and humanity can finally turn the page on this ugly pandemic and focus on other matters, for e.g. progressive and meaningful development, standards of education and teaching, enhanced living experience, shared values in a unified civilisation, among others.
Réflexion
This is a very stressful and testing time for not only the academic community but also to the rest of the human population and until the planet is immunised and reliable treatments made accessible to all, we cannot lower our guards or act recklessly towards this dangerous and deadly virus.

We must NEVER FORGET that there is a deadly virus circulating and any minor slip or even a small reflex [e.g. scratching the eyelids] can mean death. We must follow the barrier moves at all times and be incredibly conscious of our every move and actions while also constantly maintaining a strict clinical hygiene. Those who are not following these protective rules are not only playing with their own life but with those of others and a good suggestion for these dangerous, irresponsible and immature people would be to imagine 2,700,000 human corpses stacked in a heap in front of them and ask themselves whether they would like to be part of it, because this is the number of lives the CoVID-19 epidemic has claimed in a few months which includes many highly trained and experienced doctors.

Image: Skulls in the Opdas mass burial cave (for illustrative purposes only)
We have also heard and read some rumours in the media regarding the impact of weather and climate on the COVID-19 pandemic. What a recent study in Science (Baker et al., 2020) found is that humid climates tend to favour stronger outbreaks, however summer and sunshine will not limit the pandemic growth substantially. The only things that will give us all our life back are effective antivirals and a reliable and safe vaccine with proven long-term efficacy successfully distributed and administered as fast as possible to immunise the human population.
It is also understandable that many people are also eager to get back to resuming their normal lives and having been confined for so long many want to travel or go on holidays, especially confined couples.

Image: Lady in red / A.Lloyd
However, it is imperative to understand that as long as effective antivirals are not made accessible worldwide and vaccination campaigns are not completed, this incredibly dangerous virus will continue circulating among human populations on the planet. Hence, as matters currently stand the wisest behaviour for the time being is to wait and be patient while also minimising unimportant social interactions and travel and only focus on what is truly important. We should only leave the house for essential and vital reasons such as for work [if impossible to work from home] and for food provisions. The severe acute respiratory syndrome COVID-19 / Coronavirus II (SARS-CoV-2) pandemic is a powerful reminder of the ability of infectious diseases to sicken, kill and disrupt, even in the most technologically advanced generation.
Video: Une note sur le COVID 19 et la gestion de la civilisation [En Francais & in English (Starts at 13:00)]
I would also like to thank all my readers, followers and supporters for their kindness, time, loyalty and trust. It will soon be almost a decade since dpurb.com was launched and we have been through so much together, in many cases all of us behind our screens but travelling the universe, living, experiencing so much within our minds.
Since launching dpurb.com in 2012 I have met so many people from England, France and other places, from all walks of life (in offices, universities, libraries, on the internet, in art galleries, on the streets, etc) who have sometimes asked me some great questions to which I have most of the time answered by speeches that have always been well received and admired; so I recently decided to put all those answers in writing so that the whole world can understand, feel and connect with our line of thought, values, philosophy and goals [These can be found in the essay « Top XV Questions asked by French & English people over the years »].
I shall end this essay by emphasising on the fact that dpurb.com was launched with the firm intention to touch, inspire and motivate individuals from all walks of life that make up our human civilisation on our little planet Earth, from the small to the immense.
Sincerely,
Danny d’Purb
Note: We can also be followed on Twitter: @DannyDPurb
Le Boléro de Ravel par l’Orchestre national de France en #confinement #ensembleàlamaison
(FR) Vous trouverez ci-dessous une liste des principaux articles relatifs à la crise COVID-19 en cours. La liste ci-dessous sera continuellement mise à jour comme tous nos articles sur le site. Veuillez visiter ce poste périodiquement pour plus d’informations pendant que nous luttons ensemble contre cet horrible virus en tant qu’une civilisation des créatures les plus intelligentes de la Terre.
(EN) Below is a list of the top articles related to the ongoing COVID-19 crisis. The list below will be continuously updated as all of our posts on the website. Please visit this post periodically for more information as we fight this ugly virus together as a civilisation of the smartest creatures on Earth.
*****
Références (Études Scientifiques) – Cliquez sur les liens
- Ahmed, S., Quadeer, A. and McKay, M., (2020). Preliminary Identification of Potential Vaccine Targets for the COVID-19 Coronavirus (SARS-CoV-2) Based on SARS-CoV Immunological Studies. Viruses, 12(3), p.254.
- Akatsu, T., (2020). The Body Vs. Coronavirus. The battle inside us (Documentary). NHK. Japan.
- Aljofan, M. and Gaipov, A., (2020). COVID-19 Treatment: The Race Against Time. Electronic Journal of General Medicine, 17(6).
- Amuasi, J., Walzer, C., Heymann, D., Carabin, H., Huong, L., Haines, A. and Winkler, A., (2020). Calling for a COVID-19 One Health Research Coalition. The Lancet.
- Aran, D. (2021). Estimating real-world COVID-19 vaccine effectiveness in Israel using aggregated counts.
- Asian Pacific Journal of Allergy and Immunology, (2020). Immune responses in COVID-19 and potential vaccines: Lessons learned from SARS and MERS epidemic.
- Baker, R., Yang, W., Vecchi, G., Metcalf, C. and Grenfell, B., (2020). Susceptible supply limits the role of climate in the early SARS-CoV-2 pandemic. Science, p.eabc2535.
- Bennardo, F., Buffone, C. and Giudice, A., (2020). New therapeutic opportunities for COVID-19 patients with Tocilizumab: Possible correlation of interleukin-6 receptor inhibitors with osteonecrosis of the jaws. Oral Oncology, p.104659.
- Bergin, C., Browne, P., Murray, P., O’Dwyer, M., Conlon, N., Kane, D., Laffey, J., Ní Choitir, C., Adams, R., O’Leary, A., King, F. and Gilvarry, P., (2020). Interim Guidance For The Use Of Tocilizumab In The Management Of Patients Who Have Severe COVID-19 With Suspected Hyperinflammation [V3.0]. The Irish Health Repository.
- Bernal, J., Andrews, N., Gower, C., Stowe, J., Robertson, C., and Tessier, E. et al. (2021). Early effectiveness of COVID-19 vaccination with BNT162b2 mRNA vaccine and ChAdOx1 adenovirus vector vaccine on symptomatic disease, hospitalisations and mortality in older adults in England.
- Bi, Q., Wu, Y., Mei, S., Ye, C., Zou, X., Zhang, Z., Liu, X., Wei, L., Truelove, S., Zhang, T., Gao, W., Cheng, C., Tang, X., Wu, X., Wu, Y., Sun, B., Huang, S., Sun, Y., Zhang, J., Ma, T., Lessler, J. and Feng, T., (2020). Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: a retrospective cohort study. The Lancet Infectious Diseases,.
- Boytchev, H. (2021). Why did a German newspaper insist the Oxford AstraZeneca vaccine was inefficacious for older people—without evidence?. BMJ n414.
- Buchbinder, S., McElrath, M., Dieffenbach, C. and Corey, L., (2020). Use of adenovirus type-5 vectored vaccines: a cautionary tale. The Lancet, 396(10260), pp.e68-e69.
- Carsetti, R., Quintarelli, C., Quinti, I., Piano Mortari, E., Zumla, A., Ippolito, G. and Locatelli, F., (2020). The immune system of children: the key to understanding SARS-CoV-2 susceptibility?. The Lancet Child & Adolescent Health,.
- Cellina, M., Orsi, M., Bombaci, F., Sala, M., Marino, P. and Oliva, G., (2020). Favorable changes of CT findings in a patient with COVID-19 pneumonia after treatment with tocilizumab. Diagnostic and Interventional Imaging,.
- Challen, R., Brooks-Pollock, E., Read, J., Dyson, L., Tsaneva-Atanasova, K. and Danon, L., (2021). Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: matched cohort study. BMJ, p.n579.
- Challender, D., Harrop, S. and MacMillan, D., (2015). Understanding markets to conserve trade-threatened species in CITES. Biological Conservation, 187, pp.249-259.
- Chang, R. and Sun, W., (2020). Repositioning Chloroquine as Ideal Antiviral Prophylactic against COVID-19 – Time is Now.
- Chen, L., Liu, H., Liu, W., Liu, J., Liu, K., Shang, J., Deng, Y. and Wei, S., (2020). [Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia]. Chinese Journal of Tuberculosis and Respiratory, 43(0):E005.
- Chen, L., Xiong, J., Bao, L. and Shi, Y., (2020). Convalescent plasma as a potential therapy for COVID-19. The Lancet Infectious Diseases, 20(4), pp.398-400.
- Chodick, G., Tene, L., Patalon, T., Gazit, S., Tov, A., and Cohen, D. et al. (2021). The effectiveness of the first dose of BNT162b2 vaccine in reducing SARS-CoV-2 infection 13-24 days after immunization: real-world evidence.
- Coffman, R., Sher, A. and Seder, R., (2010). Vaccine Adjuvants: Putting Innate Immunity to Work. Immunity, 33(4), pp.492-503.
- Collier, D., Ferreira, I., Datir, R., Meng, B., Bergamaschi, L., and Lim, E. et al. (2021). Age-related heterogeneity in neutralising antibody responses to SARS-CoV-2 following BNT162b2 vaccination.
- Colson, P., Rolain, J., Lagier, J., Brouqui, P. and Raoult, D., (2020). Chloroquine and hydroxychloroquine as available weapons to fight COVID-19. International Journal of Antimicrobial Agents, p.105932.
- Cortegiani, A., Ingoglia, G., Ippolito, M., Giarratano, A. and Einav, S., (2020). A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. Journal of Critical Care.
- Day, M., (2020). Covid-19: ibuprofen should not be used for managing symptoms, say doctors and scientists. BMJ, p.m1086.
- Day, M. (2021). Covid-19: Stronger warnings are needed to curb socialising after vaccination, say doctors and behavioural scientists. BMJ n783.
- De Luna, G., Habibi, A., Deux, J., Colard, M., d’Alexandry d’Orengiani, A., Schlemmer, F., Joher, N., Kassasseya, C., Pawlotsky, J., Ourghanlian, C., Michel, M., Mekontso-Dessap, A. and Bartolucci, P., (2020). Rapid and Severe Covid-19 Pneumonia with Severe Acute Chest Syndrome in a Sickle Cell Patient Successfully Treated with Tocilizumab. American Journal of Hematology,.
- Diao, B., Wang, C., Wang, R., Feng, Z., Tan, Y., Wang, H., Wang, C., Liu, L., Liu, Y., Liu, Y., Wang, G., Yuan, Z., Ren, L., Wu, Y. and Chen, Y., (2020). Human Kidney is a Target for Novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection.
- Dong, L., Hu, S. and Gao, J., (2020). Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discoveries & Therapeutics, 14(1), pp.58-60.
- Dyer, O., (2020). Covid-19: Many poor countries will see almost no vaccine next year, aid groups warn. BMJ, p.m4809.
- D’purb, D.,(2016). Clinical Psychology: Controversies that surround modern day mental health practice. dpurb.com essais
- D’purb, D., (2018). Clinical Psychology: Learning Disabilities, Anxiety, Depression & Schizophrenia and the Effectiveness of Psychotherapy. dpurb.com essais
- D’purb, D., (2016). History on Western Philosophy, Religious cultures, Science, Medicine & Secularisation. dpurb.com essais
- D’purb, D., (2018). Psychoanalysis: History, Foundations, Legacy, Impact & Evolution. dpurb.com essais
- D’purb, D., (2016). Psychology: The Concept of Self. dpurb.com essais
- Dogra, P., Koay, E., Wang, Z., Vahidy, F., Ferrari, M., Pasqualini, R., Arap, W., Boom, M., Sostman, H. and Cristini, V., (2021). Do Pandemics Obey the Elliott Wave Principle of Financial Markets?.
- Edara, V., Floyd, K., Lai, L., Gardner, M., Hudson, W., Piantadosi, A., Waggoner, J., Babiker, A., Ahmed, R., Xie, X., Lokugamage, K., Menachery, V., Shi, P. and Suthar, M., (2021). Infection and mRNA-1273 vaccine antibodies neutralize SARS-CoV-2 UK variant.
- Ella, R., Vadrevu, K., Jogdand, H., Prasad, S., Reddy, S., Sarangi, V., Ganneru, B., Sapkal, G., Yadav, P., Abraham, P., Panda, S., Gupta, N., Reddy, P., Verma, S., Kumar Rai, S., Singh, C., Redkar, S., Gillurkar, C., Kushwaha, J., Mohapatra, S., Rao, V., Guleria, R., Ella, K. and Bhargava, B., (2021). Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: a double-blind, randomised, phase 1 trial. The Lancet Infectious Diseases,.
- Ella, R., Reddy, S., Jogdand, H., Sarangi, V., Ganneru, B., Prasad, S., Das, D., Raju, D., Praturi, U., Sapkal, G., Yadav, P., Reddy, P., Verma, S., Singh, C., Redkar, S., Gillurkar, C., Kushwaha, J., Mohapatra, S., Bhate, A., Rai, S., Panda, S., Abraham, P., Gupta, N., Ella, K., Bhargava, B. and Vadrevu, K., 2021. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: interim results from a double-blind, randomised, multicentre, phase 2 trial, and 3-month follow-up of a double-blind, randomised phase 1 trial. The Lancet Infectious Diseases,.
- Emary, K., Golubchik, T., Aley, P., Ariani, C., Angus, B., Bibi, S., Blane, B., Bonsall, D., Cicconi, P., Charlton, S., Clutterbuck, E., Collins, A., Cox, T., Darton, T., Dold, C., Douglas, A., Duncan, C., Ewer, K., Flaxman, A., Faust, S., Ferreira, D., Feng, S., Finn, A., Folegatti, P., Fuskova, M., Galiza, E., Goodman, A., Green, C., Green, C., Greenland, M., Hallis, B., Heath, P., Hay, J., Hill, H., Jenkin, D., Kerridge, S., Lazarus, R., Libri, V., Lillie, P., Ludden, C., Marchevsky, N., Minassian, A., McGregor, A., Farooq Mujadidi, Y., Phillips, D., Plested, E., Pollock, K., Robinson, H., Smith, A., Song, R., Snape, M., Sutherland, R., Thomson, E., Toshner, M., Turner, D., Vekemans, J., Villafana, T., Williams, C., Hill, A., Lambe, T., Gilbert, S., Voysey, M., Ramasamy, M., Pollard, A. and Group, O., (2021). Efficacy of ChAdOx1 nCoV-19 (AZD1222) Vaccine Against SARS-CoV-2 VOC 202012/01 (B.1.1.7). SSRN Electronic Journal,.
- Evans, R., McAuley, H., Harrison, E., Shikotra, A., Singapuri, A., Sereno, M., Elneima, O., Docherty, A., Lone, N., Leavy, O., Daines, L., Baillie, J., Brown, J., Chalder, T., De Soyza, A., Diar Bakerly, N., Easom, N., Geddes, J., Greening, N., Hart, N., Heaney, L., Heller, S., Howard, L., Jacob, J., Jenkins, R., Jolley, C., Kerr, S., Kon, O., Lewis, K., Lord, J., McCann, G., Neubauer, S., Openshaw, P., Pfeffer, P., Rowland, M., Semple, M., Singh, S., Sheikh, A., Thomas, D., Toshner, M., Chalmers, J., Ho, L., Horsley, A., Marks, M., Poinasamy, K., Wain, L. and Brightling, C., (2021). Physical, cognitive and mental health impacts of COVID-19 following hospitalisation – a multi-centre prospective cohort study.
- Fan, Z., Chen, L., Li, J., Tian, C., Zhang, Y., Huang, S., Liu, Z. and Cheng, J., (2020). Clinical Features of COVID-19 Related Liver Damage.
- Fazzi, E. and Galli, J., (2020). New clinical needs and strategies for care in children with neurodisability during COVID‐19. Developmental Medicine & Child Neurology,.
- Fischer, R., van Doremalen, N., Adney, D., Yinda, C., Port, J., Holbrook, M., Schulz, J., Williamson, B., Thomas, T., Barbian, K., Anzick, S., Ricklefs, S., Smith, B., Long, D., Martens, C., Saturday, G., de Wit, E., Gilbert, S., Lambe, T. and Munster, V., (2021). ChAdOx1 nCoV-19 (AZD1222) protects hamsters against SARS-CoV-2 B.1.351 and B.1.1.7 disease.
- Folegatti, P., Ewer, K., Aley, P., Angus, B., Becker, S., and Belij-Rammerstorfer, S. et al. (2020). Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial. The Lancet 396: 467-478.
- Fontana, F., Alfano, G., Mori, G., Amurri, A., Lorenzo, T., Ballestri, M., Leonelli, M., Facchini, F., Damiano, F., Magistroni, R. and Cappelli, G., (2020). Covid‐19 pneumonia in a kidney transplant recipient successfully treated with Tocilizumab and Hydroxychloroquine. American Journal of Transplantation,.
- Fu, B., Xu, X. and Wei, H., (2020). Why tocilizumab could be an effective treatment for severe COVID-19?. Journal of Translational Medicine, 18(1).
- Funk, C., Laferrière, C., and Ardakani, A. (2021). Target Product Profile Analysis of COVID-19 Vaccines in Phase III Clinical Trials and Beyond: An Early 2021 Perspective. Viruses 13: 418.
- Garçon, N., Segal, L., Tavares, F. and Van Mechelen, M., (2011). The safety evaluation of adjuvants during vaccine development: The AS04 experience. Vaccine, 29(27), pp.4453-4459.
- Gao, J., Tian, Z. and Yang, X., (2020). Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. BioScience Trends, 14(1), pp.72-73.
- Gao, Q., Bao, L., Mao, H., Wang, L., Xu, K., Yang, M., Li, Y., Zhu, L., Wang, N., Lv, Z., Gao, H., Ge, X., Kan, B., Hu, Y., Liu, J., Cai, F., Jiang, D., Yin, Y., Qin, C., Li, J., Gong, X., Lou, X., Shi, W., Wu, D., Zhang, H., Zhu, L., Deng, W., Li, Y., Lu, J., Li, C., Wang, X., Yin, W., Zhang, Y. and Qin, C., (2020). Development of an inactivated vaccine candidate for SARS-CoV-2. Science, p.eabc1932.
- Garg, S., Kim, L., Whitaker, M., O’Halloran, A., Cummings, C., Holstein, R., Prill, M., Chai, S., Kirley, P., Alden, N., Kawasaki, B., Yousey-Hindes, K., Niccolai, L., Anderson, E., Openo, K., Weigel, A., Monroe, M., Ryan, P., Henderson, J., Kim, S., Como-Sabetti, K., Lynfield, R., Sosin, D., Torres, S., Muse, A., Bennett, N., Billing, L., Sutton, M., West, N., Schaffner, W., Talbot, H., Aquino, C., George, A., Budd, A., Brammer, L., Langley, G., Hall, A. and Fry, A., (2020). Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019 — COVID-NET, 14 States, March 1–30, 2020. Morbidity and Mortality Weekly Report, 69(15), pp.458-464.
- Guo, C., Li, B., Ma, H., Wang, X., Cai, P., Yu, Q., Zhu, L., Jin, L., Jiang, C., Fang, J., Liu, Q., Zong, D., Zhang, W., Lu, Y., Li, K., Gao, X., Fu, B., Liu, L., Ma, X., Weng, J., Wei, H., Jin, T., Lin, J. and Qu, K., (2020). Tocilizumab treatment in severe COVID-19 patients attenuates the inflammatory storm incited by monocyte centric immune interactions revealed by single-cell analysis.
- Hamzavi, I., Lyons, A., Kohli, I., Narla, S., Parks-Miller, A., Gelfand, J., Lim, H. and Ozog, D., 2020. Ultraviolet germicidal irradiation: Possible method for respirator disinfection to facilitate reuse during the COVID-19 pandemic. Journal of the American Academy of Dermatology, 82(6), pp.1511-1512.
- Hu, Z., Song, C., Xu, C., Jin, G., Chen, Y., Xu, X., Ma, H., Chen, W., Lin, Y., Zheng, Y., Wang, J., Hu, Z., Yi, Y. and Shen, H., (2020). Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Science China Life Sciences.
- Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., Zhang, L., Fan, G., Xu, J., Gu, X., Cheng, Z., Yu, T., Xia, J., Wei, Y., Wu, W., Xie, X., Yin, W., Li, H., Liu, M., Xiao, Y., Gao, H., Guo, L., Xie, J., Wang, G., Jiang, R., Gao, Z., Jin, Q., Wang, J. and Cao, B., (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), pp.497-506.
- Hunter, P., and Brainard, J. (2021). Estimating the effectiveness of the Pfizer COVID-19 BNT162b2 vaccine after a single dose. A reanalysis of a study of ‘real-world’ vaccination outcomes from Israel.
- Iacobucci, G., and Mahase, E. (2021). Covid-19 vaccination: What’s the evidence for extending the dosing interval?. BMJ n18.
- Jain, J., Saurabh, S., Goel, A., Gupta, M., Bhardwaj, P., and Raghav, P. (2021). COVID-19 vaccine hesitancy among undergraduate medical students: results from a nationwide survey in India.
- Jiménez-Antón, M., Grau, M., Olías-Molero, A. and Alunda, J., (2019). Syrian Hamster as an Advanced Experimental Model for Visceral Leishmaniasis. Methods in Molecular Biology, pp.303-314.
- Jayadevan, R., Shenoy, R., and TS, A. (2021). Survey of symptoms following COVID-19 vaccination in India.
- Jin, Z., Zhao, Y., Sun, Y., Zhang, B., Wang, H., Wu, Y., Zhu, Y., Zhu, C., Hu, T., Du, X., Duan, Y., Yu, J., Yang, X., Yang, X., Yang, K., Liu, X., Guddat, L., Xiao, G., Zhang, L., Yang, H. and Rao, Z., (2020). Structural basis for the inhibition of SARS-CoV-2 main protease by antineoplastic drug carmofur. Nature Structural & Molecular Biology,.
- Juan, J., Gil, M., Rong, Z., Zhang, Y., Yang, H. and Poon, L., (2020). Effects of Coronavirus Disease 2019 (COVID-19) on Maternal, Perinatal and Neonatal Outcomes: a Systematic Review of 266 Pregnancies.
- Karlsson, L., Soveri, A., Lewandowsky, S., Karlsson, L., Karlsson, H., and Nolvi, S. et al. (2021). Fearing the disease or the vaccine: The case of COVID-19. Personality And Individual Differences 172: 110590.
- Kearney, J., (2020). Chloroquine as a Potential Treatment and Prevention Measure for the 2019 Novel Coronavirus: A Review.
- Kim, Y., Dema, B. and Reyes-Sandoval, A., (2020). COVID-19 vaccines: breaking record times to first-in-human trials. npj Vaccines, 5(1).
- Klok, F., Kruip, M., van der Meer, N., Arbous, M., Gommers, D., Kant, K., Kaptein, F., van Paassen, J., Stals, M., Huisman, M. and Endeman, H., (2020). Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thrombosis Research,.
- Kmietowicz, Z., (2015). Processed meats are carcinogenic, says new review of evidence. BMJ, p.h5729.
- Kim, J., Marks, F. and Clemens, J., (2021). Looking beyond COVID-19 vaccine phase 3 trials. Nature Medicine, 27(2), pp.205-211.
- Kong, W., Li, Y., Peng, M., Kong, D., Yang, X., Wang, L. and Liu, M., (2020). SARS-CoV-2 detection in patients with influenza-like illness. Nature Microbiology, 5(5), pp.675-678.
- Konno, Y., Kimura, I., Uriu, K., Fukushi, M., Irie, T., and Koyanagi, Y. et al. (2020). SARS-CoV-2 ORF3b Is a Potent Interferon Antagonist Whose Activity Is Increased by a Naturally Occurring Elongation Variant. Cell Reports 32: 108185.
- Krumrei-Mancuso, E., Haggard, M., LaBouff, J. and Rowatt, W. (2019). Links between intellectual humility and acquiring knowledge. The Journal of Positive Psychology, 15(2), pp.155-170.
- Lamers, M., Beumer, J., van der Vaart, J., Knoops, K., Puschhof, J., Breugem, T., Ravelli, R., Paul van Schayck, J., Mykytyn, A., Duimel, H., van Donselaar, E., Riesebosch, S., Kuijpers, H., Schippers, D., van de Wetering, W., de Graaf, M., Koopmans, M., Cuppen, E., Peters, P., Haagmans, B. and Clevers, H., (2020). SARS-CoV-2 productively infects human gut enterocytes. Science, p.eabc1669.
- Letko, M., Miazgowicz, K., McMinn, R., Seifert, S., Sola, I., Enjuanes, L., Carmody, A., van Doremalen, N. and Munster, V., (2018). Adaptive Evolution of MERS-CoV to Species Variation in DPP4. Cell Reports, 24(7), pp.1730-1737.
- Leung, N., Chu, D., Shiu, E., Chan, K., McDevitt, J., Hau, B., Yen, H., Li, Y., Ip, D., Peiris, J., Seto, W., Leung, G., Milton, D. and Cowling, B., (2020). Respiratory virus shedding in exhaled breath and efficacy of face masks. Nature Medicine,.
- Li, Z., Wu, M., Yao, J., Guo, J., Liao, X., Song, S., Li, J., Duan, G., Zhou, Y., Wu, X., Zhou, Z., Wang, T., Hu, M., Chen, X., Fu, Y., Lei, C., Dong, H., Xu, C., Hu, Y., Han, M., Zhou, Y., Jia, H., Chen, X. and Yan, J., (2020). Caution on Kidney Dysfunctions of COVID-19 Patients.
- Liu, J., Cao, R., Xu, M., Wang, X., Zhang, H., Hu, H., Li, Y., Hu, Z., Zhong, W. and Wang, M., (2020). Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection in vitro. Cell Discovery, 6(1).
- Liu, Y., Liu, J., Xia, H., Zhang, X., Fontes-Garfias, C., Swanson, K., Cai, H., Sarkar, R., Chen, W., Cutler, M., Cooper, D., Weaver, S., Muik, A., Sahin, U., Jansen, K., Xie, X., Dormitzer, P. and Shi, P., (2021). Neutralizing Activity of BNT162b2-Elicited Serum. New England Journal of Medicine,.
- Logunov, D., Dolzhikova, I., Zubkova, O., Tukhvatulin, A., Shcheblyakov, D., and Dzharullaeva, A. et al. (2020). Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: two open, non-randomised phase 1/2 studies from Russia. The Lancet 396: 887-897.
- Logunov, D., Dolzhikova, I., Shcheblyakov, D., Tukhvatulin, A., Zubkova, O., and Dzharullaeva, A. et al. (2021). Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: an interim analysis of a randomised controlled phase 3 trial in Russia. The Lancet 397: 671-681.
- Loo, K., Letchumanan, V., Ser, H., Teoh, S., Law, J., Tan, L., Ab Mutalib, N., Chan, K. and Lee, L., (2021). COVID-19: Insights into Potential Vaccines. Microorganisms, 9(3), p.605.
- Lu, S. (2009). Heterologous prime–boost vaccination. Current Opinion In Immunology 21: 346-351.
- Lu, C., Chen, M. and Chang, Y., (2020). Potential therapeutic agents against COVID-19. Journal of the Chinese Medical Association, p.1.
- Lurie, N., Saville, M., Hatchett, R. and Halton, J., (2020). Developing Covid-19 Vaccines at Pandemic Speed. New England Journal of Medicine.
- Madhi, S., Baillie, V., Cutland, C., Voysey, M., Koen, A., Fairlie, L., Padayachee, S., Dheda, K., Barnabas, S., Bhorat, Q., Briner, C., Kwatra, G., Ahmed, K., Aley, P., Bhikha, S., Bhiman, J., Bhorat, A., du Plessis, J., Esmail, A., Groenewald, M., Horne, E., Hwa, S., Jose, A., Lambe, T., Laubscher, M., Malahleha, M., Masenya, M., Masilela, M., McKenzie, S., Molapo, K., Moultrie, A., Oelofse, S., Patel, F., Pillay, S., Rhead, S., Rodel, H., Rossouw, L., Taoushanis, C., Tegally, H., Thombrayil, A., van Eck, S., Wibmer, C., Durham, N., Kelly, E., Villafana, T., Gilbert, S., Pollard, A., de Oliveira, T., Moore, P., Sigal, A. and Izu, A., (2021). Efficacy of the ChAdOx1 nCoV-19 Covid-19 Vaccine against the B.1.351 Variant. New England Journal of Medicine,.
- Mao, L., Jin, H., Wang, M., Hu, Y., Chen, S., He, Q., Chang, J., Hong, C., Zhou, Y., Wang, D., Miao, X., Li, Y. and Hu, B., (2020). Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurology.
- Mahase, E., (2020). Covid-19: what treatments are being investigated?. BMJ, p.m1252.
- Mahase, E. (2021). Covid-19: UK approves Moderna vaccine to be given as two doses 28 days apart. BMJ n74.
- Mahase, E. (2021). How the Oxford-AstraZeneca covid-19 vaccine was made. BMJ n86.
- Mahase, E. (2021). Covid-19: Novavax vaccine efficacy is 86% against UK variant and 60% against South African variant. BMJ n296.
- Mihai, C., Dobrota, R., Schröder, M., Garaiman, A., Jordan, S., Becker, M., Maurer, B. and Distler, O., (2020). COVID-19 In A Patient With Systemic Sclerosis Treated With Tocilizumab For Ssc-ILD. Annals of Rheumatic Diseases, 79(5).
- Miller, A., Reandelar, M., Fasciglione, K., Roumenova, V., Li, Y. and Otazu, G., (2020). Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study.
- Moazzen, N., Imani, B., Aelami, M., Motevali, N., Kianifar, H., Khoushkhui, M. and Ahancian, H., (2020). How to boost your immune system against Coronavirus infection?. Arch Bone Jt Surg, 8(1).
- Moghadas, S., Vilches, T., Zhang, K., Nourbakhsh, S., Sah, P., and Fitzpatrick, M. et al. (2021). Evaluation of COVID-19 vaccination strategies with a delayed second dose.
- Moodie, Z., Metch, B., Bekker, L., Churchyard, G., Nchabeleng, M., Mlisana, K., Laher, F., Roux, S., Mngadi, K., Innes, C., Mathebula, M., Allen, M., Bentley, C., Gilbert, P., Robertson, M., Kublin, J., Corey, L. and Gray, G., (2015). Continued Follow-Up of Phambili Phase 2b Randomized HIV-1 Vaccine Trial Participants Supports Increased HIV-1 Acquisition among Vaccinated Men. PLOS ONE, 10(9), p.e0137666.
- Moriguchi, T., Harii, N., Goto, J., Harada, D., Sugawara, H., Takamino, J., Ueno, M., Sakata, H., Kondo, K., Myose, N., Nakao, A., Takeda, M., Haro, H., Inoue, O., Suzuki-Inoue, K., Kubokawa, K., Ogihara, S., Sasaki, T., Kinouchi, H., Kojin, H., Ito, M., Onishi, H., Shimizu, T., Sasaki, Y., Enomoto, N., Ishihara, H., Furuya, S., Yamamoto, T. and Shimada, S., (2020). A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. International Journal of Infectious Diseases, 94, pp.55-58.
- Muik, A., Wallisch, A., Sänger, B., Swanson, K., Mühl, J., Chen, W., Cai, H., Maurus, D., Sarkar, R., Türeci, Ö., Dormitzer, P. and Şahin, U., (2021). Neutralization of SARS-CoV-2 lineage B.1.1.7 pseudovirus by BNT162b2 vaccine–elicited human sera. Science, 371(6534), pp.1152-1153.
- Mulligan, M., Lyke, K., Kitchin, N., Absalon, J., Gurtman, A., and Lockhart, S. et al. (2020). Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 586: 589-593.
- Muñoz-Fontela, C., Dowling, W., Funnell, S., Gsell, P., Riveros-Balta, A., Albrecht, R., Andersen, H., Baric, R., Carroll, M., Cavaleri, M., Qin, C., Crozier, I., Dallmeier, K., de Waal, L., de Wit, E., Delang, L., Dohm, E., Duprex, W., Falzarano, D., Finch, C., Frieman, M., Graham, B., Gralinski, L., Guilfoyle, K., Haagmans, B., Hamilton, G., Hartman, A., Herfst, S., Kaptein, S., Klimstra, W., Knezevic, I., Krause, P., Kuhn, J., Le Grand, R., Lewis, M., Liu, W., Maisonnasse, P., McElroy, A., Munster, V., Oreshkova, N., Rasmussen, A., Rocha-Pereira, J., Rockx, B., Rodríguez, E., Rogers, T., Salguero, F., Schotsaert, M., Stittelaar, K., Thibaut, H., Tseng, C., Vergara-Alert, J., Beer, M., Brasel, T., Chan, J., García-Sastre, A., Neyts, J., Perlman, S., Reed, D., Richt, J., Roy, C., Segalés, J., Vasan, S., Henao-Restrepo, A. and Barouch, D., (2020). Animal models for COVID-19. Nature, 586(7830), pp.509-515.
- Oberemok, V., Laikova, K., Yurchenko, K., Fomochkina, I. and Kubyshkin, A., (2020). SARS-CoV-2 will continue to circulate in the human population: an opinion from the point of view of the virus-host relationship. Inflammation Research,.
- Paltiel, A., Schwartz, J., Zheng, A., and Walensky, R. (2021). Clinical Outcomes Of A COVID-19 Vaccine: Implementation Over Efficacy. Health Affairs 40: 42-52.
- Parvin, F., Islam, S., Urmy, Z., & Ahmed, S. (2020). THE SYMPTOMS, CONTAGIOUS PROCESS, PREVENTION AND POST TREATMENT OF COVID-19. European Journal of Physiotherapy and Rehabilitation Studies, 0. Retrieved from https://www.oapub.org/hlt/index.php/EJPRS/article/view/52
- Patel SK, Pathak M, Tiwari R, Yatoo MI, Malik YS, Sah R, Rabaan AA, Sharun K, Dhama K, Bonilla-Aldana DK, Rodriguez-Morales AJ. (2020). A vaccine is not too far for COVID-19. J Infect Dev Ctries
- Patruno, C., Stingeni, L., Fabbrocini, G., Hansel, K. and Napolitano, M., (2020). Dupilumab and COVID ‐19: what should we expect?. Dermatologic Therapy,.
- Polack, F., Thomas, S., Kitchin, N., Absalon, J., Gurtman, A., and Lockhart, S. et al. (2020). Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. New England Journal Of Medicine 383: 2603-2615.
- Porter, T. and Schumann, K. (2017). Intellectual humility and openness to the opposing view. Self and Identity, 17(2), pp.139-162.
- Robbiani, D., Gaebler, C., Muecksch, F., Lorenzi, J., Wang, Z., and Cho, A. et al. (2020). Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Nature 584: 437-442.
- Robertson, J., Sewell, H., and Stewart, M. (2021). Delayed second dose of the BNT162b2 vaccine: innovation or misguided conjecture?. The Lancet 397: 879-880.
- Rosen, B., Waitzberg, R. and Israeli, A., (2021). Israel’s rapid rollout of vaccinations for COVID-19. Israel Journal of Health Policy Research, 10(1).
- Rosenbloom, D. and Markard, J., (2020). A COVID-19 recovery for climate. Science, 368(6490), pp.447-447.
- Rostad, C. and Anderson, E., (2021). Optimism and caution for an inactivated COVID-19 vaccine. The Lancet Infectious Diseases,.
- SaifAddin, B., Almogbel, A., Zollner, C., Wu, F., Bonef, B., Iza, M., Nakamura, S., DenBaars, S. and Speck, J., (2020). AlGaN Deep-Ultraviolet Light-Emitting Diodes Grown on SiC Substrates. ACS Photonics, 7(3), pp.554-561.
- Sallam, M. (2021). COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 9: 160.
- Santos, I., Grosche, V., Sabino-Silva, R. and Jardim, A., (2020). Antivirals against human and animal Coronaviruses: different approach in SARS-CoV-2 treatment.
- Schleicher, G., Lowman, W. and Richards, G., (2020). Case Study: A Patient with Asthma, Covid-19 Pneumonia and Cytokine Release Syndrome Treated with Corticosteroids and Tocilizumab. Wits Journal of Clinical Medicine, 2(SI), p.47.
- Schrack, J., Wanigatunga, A. and Juraschek, S., (2020). After the COVID-19 Pandemic: The Next Wave of Health Challenges for Older Adults. The Journals of Gerontology: Series A,.
- Shenker, N., Aprigio, J., Arslanoglu, S., Aye, N., Bærug, A., Bar Yam, N., Barnett, D., Bellad, R., Bertino, E., Bethou, A., Bharadva, K., Olin, A., Billeaud, C., Buffin, R., Cassidy, T., Chugh Sachdeva, R., Clifford, V., Coutsoudis, A., Deb, S., Domjan, A., Fang, L., Festival, J., Franks, A., Garcia-Lara, N., Gaya, A., Golubiú-Úepuliú, B., Groff, L., Grøvslien, A., Hamilton Spence, E., Heidarzadeh, M., Hosseini, M., Hughes, J., Israel-Ballard, K., Jain, K., Jain, S., Jayaraman, S., Jones, F., Kale, P., Kasar, J., Kithua, A., Klein, L., Klotz, D., Lin, Y., Liu, X., Lockhart Borman, L., Lundstrom, J., Malzacher, A., Mansen, K., Mathisen, R., Mileusnic-Milenovic, R., Moe, Z., Moro, G., Mukherjee, S., Myint, S., Nangia, S., Ngerncham, S., Njeru, F., Olonan-Jusi, E., Opie, G., Palmquist, A., Reimers, P., Saboute, M., Sakamoto, P., Sanchez, S., Shenker, N., Singh, H., Singh, J., Singh, P., Staff, M., Sulfaro, C., Thi Hoang, T., Tiit-Vesingi, A., Tiwari, S., van Goudoever, J., Vickers, A., Waiyego, M., Weaver, G., Wesolowska, A. and Wright, J., (2020). Maintaining safety and service provision in human milk banking: a call to action in response to the COVID-19 pandemic. The Lancet Child & Adolescent Health,.
- Shi, J., Wen, Z., Zhong, G., Yang, H., Wang, C., Huang, B., Liu, R., He, X., Shuai, L., Sun, Z., Zhao, Y., Liu, P., Liang, L., Cui, P., Wang, J., Zhang, X., Guan, Y., Tan, W., Wu, G., Chen, H. and Bu, Z., (2020). Susceptibility of ferrets, cats, dogs, and other domesticated animals to SARS–coronavirus 2. Science, p.eabb7015.
- Shi, S., Qin, M., Shen, B., Cai, Y., Liu, T., Yang, F., Gong, W., Liu, X., Liang, J., Zhao, Q., Huang, H., Yang, B. and Huang, C., (2020). Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiology,.
- Sigfrid, L., Drake, T., Pauley, E., Jesudason, E., Olliaro, P., Lim, W., Gillesen, A., Berry, C., Lowe, D., McPeake, J., Lone, N., Cevik, M., Munblit, D., Casey, A., Bannister, P., Russell, C., Goodwin, L., Ho, A., Turtle, L., O’Hara, M., Hastie, C., Donohue, C., Spencer, R., Harrison, J., Donegan, C., Gummery, A., Hardwick, H., Hastie, C., Merson, L., Carson, G., Kenneth Baillie, J., Openshaw, P., Harrison, E., Docherty, A., Semple, M. and Scott, J., (2021). Long Covid in adults discharged from UK hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO Clinical Characterisation Protocol.
- Srivastava, N. and Saxena, S., (2020). Prevention and Control Strategies for SARS-CoV-2 Infection. Medical Virology: From Pathogenesis to Disease Control, pp.127-140.
- Stadnytskyi, V., Bax, C., Bax, A. and Anfinrud, P., (2020). The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proceedings of the National Academy of Sciences, p.202006874.
- Sun, P., Lu, X., Xu, C., Sun, W. and Pan, B., (2020). Understanding of COVID‐19 based on current evidence. Journal of Medical Virology.
- Tada, T., Dcosta, B., Samanovic-Golden, M., Herati, R., Cornelius, A., Mulligan, M. and Landau, N., (2021). Neutralization of viruses with European, South African, and United States SARS-CoV-2 variant spike proteins by convalescent sera and BNT162b2 mRNA vaccine-elicited antibodies.
- Taipale, J., Romer, P. and Linnarsson, S., (2020). Population-scale testing can suppress the spread of COVID-19.
- Thiagarajan, K. (2021). Covid-19: India is at centre of global vaccine manufacturing, but opacity threatens public trust. BMJ n196.
- Thorp, H., (2020). Do us a favor. Science, 367(6483), pp.1169-1169.
- Thorp, H., (2020). Time to pull together. Science, 367(6484), pp.1282-1282.
- Tinari, S., (2021). The EMA covid-19 data leak, and what it tells us about mRNA instability. BMJ, p.n627.
- Torjesen, I. (2021). Covid-19: First doses of vaccines in Scotland led to a substantial fall in hospital admissions. BMJ n523.
- van Kraaij, T., Mostard, R., Ramiro, S., Magro Checa, C., van Dongen, C., van Haren, E., Buijs, J., & Landewé, R. (2020). Tocilizumab in Severe COVID-19 Pneumonia and Concomitant Cytokine Release Syndrome. European Journal of Case Reports in Internal Medicine, 2.
- Vidyasagar, V. and Nithish, C., (2020). Convalescentplasma as potential therapy for recently emerged novel CoVID-19. EPRA International Journal of Research & Development (IJRD), 5(4).
- Voysey, M., Clemens, S., Madhi, S., Weckx, L., Folegatti, P., Aley, P., Angus, B., Baillie, V., Barnabas, S., Bhorat, Q., Bibi, S., Briner, C., Cicconi, P., Collins, A., Colin-Jones, R., Cutland, C., Darton, T., Dheda, K., Duncan, C., Emary, K., Ewer, K., Fairlie, L., Faust, S., Feng, S., Ferreira, D., Finn, A., Goodman, A., Green, C., Green, C., Heath, P., Hill, C., Hill, H., Hirsch, I., Hodgson, S., Izu, A., Jackson, S., Jenkin, D., Joe, C., Kerridge, S., Koen, A., Kwatra, G., Lazarus, R., Lawrie, A., Lelliott, A., Libri, V., Lillie, P., Mallory, R., Mendes, A., Milan, E., Minassian, A., McGregor, A., Morrison, H., Mujadidi, Y., Nana, A., O’Reilly, P., Padayachee, S., Pittella, A., Plested, E., Pollock, K., Ramasamy, M., Rhead, S., Schwarzbold, A., Singh, N., Smith, A., Song, R., Snape, M., Sprinz, E., Sutherland, R., Tarrant, R., Thomson, E., Török, M., Toshner, M., Turner, D., Vekemans, J., Villafana, T., Watson, M., Williams, C., Douglas, A., Hill, A., Lambe, T., Gilbert, S., Pollard, A., Aban, M., Abayomi, F., Abeyskera, K., Aboagye, J., Adam, M., Adams, K., Adamson, J., Adelaja, Y., Adewetan, G., Adlou, S., Ahmed, K., Akhalwaya, Y., Akhalwaya, S., Alcock, A., Ali, A., Allen, E., Allen, L., Almeida, T., Alves, M., Amorim, F., Andritsou, F., Anslow, R., Appleby, M., Arbe-Barnes, E., Ariaans, M., Arns, B., Arruda, L., Azi, P., Azi, L., Babbage, G., Bailey, C., Baker, K., Baker, M., Baker, N., Baker, P., Baldwin, L., Baleanu, I., Bandeira, D., Bara, A., Barbosa, M., Barker, D., Barlow, G., Barnes, E., Barr, A., Barrett, J., Barrett, J., Bates, L., Batten, A., Beadon, K., Beales, E., Beckley, R., Belij-Rammerstorfer, S., Bell, J., Bellamy, D., Bellei, N., Belton, S., Berg, A., Bermejo, L., Berrie, E., Berry, L., Berzenyi, D., Beveridge, A., Bewley, K., Bexhell, H., Bhikha, S., Bhorat, A., Bhorat, Z., Bijker, E., Birch, G., Birch, S., Bird, A., Bird, O., Bisnauthsing, K., Bittaye, M., Blackstone, K., Blackwell, L., Bletchly, H., Blundell, C., Blundell, S., Bodalia, P., Boettger, B., Bolam, E., Boland, E., Bormans, D., Borthwick, N., Bowring, F., Boyd, A., Bradley, P., Brenner, T., Brown, P., Brown, C., Brown-O’Sullivan, C., Bruce, S., Brunt, E., Buchan, R., Budd, W., Bulbulia, Y., Bull, M., Burbage, J., Burhan, H., Burn, A., Buttigieg, K., Byard, N., Cabera Puig, I., Calderon, G., Calvert, A., Camara, S., Cao, M., Cappuccini, F., Cardoso, J., Carr, M., Carroll, M., Carson-Stevens, A., Carvalho, Y., Carvalho, J., Casey, H., Cashen, P., Castro, T., Castro, L., Cathie, K., Cavey, A., Cerbino-Neto, J., Chadwick, J., Chapman, D., Charlton, S., Chelysheva, I., Chester, O., Chita, S., Cho, J., Cifuentes, L., Clark, E., Clark, M., Clarke, A., Clutterbuck, E., Collins, S., Conlon, C., Connarty, S., Coombes, N., Cooper, C., Cooper, R., Cornelissen, L., Corrah, T., Cosgrove, C., Cox, T., Crocker, W., Crosbie, S., Cullen, L., Cullen, D., Cunha, D., Cunningham, C., Cuthbertson, F., Da Guarda, S., da Silva, L., Damratoski, B., Danos, Z., Dantas, M., Darroch, P., Datoo, M., Datta, C., Davids, M., Davies, S., Davies, H., Davis, E., Davis, J., Davis, J., De Nobrega, M., De Oliveira Kalid, L., Dearlove, D., Demissie, T., Desai, A., Di Marco, S., Di Maso, C., Dinelli, M., Dinesh, T., Docksey, C., Dold, C., Dong, T., Donnellan, F., Dos Santos, T., dos Santos, T., Dos Santos, E., Douglas, N., Downing, C., Drake, J., Drake-Brockman, R., Driver, K., Drury, R., Dunachie, S., Durham, B., Dutra, L., Easom, N., van Eck, S., Edwards, M., Edwards, N., El Muhanna, O., Elias, S., Elmore, M., English, M., Esmail, A., Essack, Y., Farmer, E., Farooq, M., Farrar, M., Farrugia, L., Faulkner, B., Fedosyuk, S., Felle, S., Feng, S., Ferreira Da Silva, C., Field, S., Fisher, R., Flaxman, A., Fletcher, J., Fofie, H., Fok, H., Ford, K., Fowler, J., Fraiman, P., Francis, E., Franco, M., Frater, J., Freire, M., Fry, S., Fudge, S., Furze, J., Fuskova, M., Galian-Rubio, P., Galiza, E., Garlant, H., Gavrila, M., Geddes, A., Gibbons, K., Gilbride, C., Gill, H., Glynn, S., Godwin, K., Gokani, K., Goldoni, U., Goncalves, M., Gonzalez, I., Goodwin, J., Goondiwala, A., Gordon-Quayle, K., Gorini, G., Grab, J., Gracie, L., Greenland, M., Greenwood, N., Greffrath, J., Groenewald, M., Grossi, L., Gupta, G., Hackett, M., Hallis, B., Hamaluba, M., Hamilton, E., Hamlyn, J., Hammersley, D., Hanrath, A., Hanumunthadu, B., Harris, S., Harris, C., Harris, T., Harrison, T., Harrison, D., Hart, T., Hartnell, B., Hassan, S., Haughney, J., Hawkins, S., Hay, J., Head, I., Henry, J., Hermosin Herrera, M., Hettle, D., Hill, J., Hodges, G., Horne, E., Hou, M., Houlihan, C., Howe, E., Howell, N., Humphreys, J., Humphries, H., Hurley, K., Huson, C., Hyder-Wright, A., Hyams, C., Ikram, S., Ishwarbhai, A., Ivan, M., Iveson, P., Iyer, V., Jackson, F., De Jager, J., Jaumdally, S., Jeffers, H., Jesudason, N., Jones, B., Jones, K., Jones, E., Jones, C., Jorge, M., Jose, A., Joshi, A., Júnior, E., Kadziola, J., Kailath, R., Kana, F., Karampatsas, K., Kasanyinga, M., Keen, J., Kelly, E., Kelly, D., Kelly, D., Kelly, S., Kerr, D., Kfouri, R., Khan, L., Khozoee, B., Kidd, S., Killen, A., Kinch, J., Kinch, P., King, L., King, T., Kingham, L., Klenerman, P., Knapper, F., Knight, J., Knott, D., Koleva, S., Lang, M., Lang, G., Larkworthy, C., Larwood, J., Law, R., Lazarus, E., Leach, A., Lees, E., Lemm, N., Lessa, A., Leung, S., Li, Y., Lias, A., Liatsikos, K., Linder, A., Lipworth, S., Liu, S., Liu, X., Lloyd, A., Lloyd, S., Loew, L., Lopez Ramon, R., Lora, L., Lowthorpe, V., Luz, K., MacDonald, J., MacGregor, G., Madhavan, M., Mainwaring, D., Makambwa, E., Makinson, R., Malahleha, M., Malamatsho, R., Mallett, G., Mansatta, K., Maoko, T., Mapetla, K., Marchevsky, N., Marinou, S., Marlow, E., Marques, G., Marriott, P., Marshall, R., Marshall, J., Martins, F., Masenya, M., Masilela, M., Masters, S., Mathew, M., Matlebjane, H., Matshidiso, K., Mazur, O., Mazzella, A., McCaughan, H., McEwan, J., McGlashan, J., McInroy, L., McIntyre, Z., McLenaghan, D., McRobert, N., McSwiggan, S., Megson, C., Mehdipour, S., Meijs, W., Mendonça, R., Mentzer, A., Mirtorabi, N., Mitton, C., Mnyakeni, S., Moghaddas, F., Molapo, K., Moloi, M., Moore, M., Moraes-Pinto, M., Moran, M., Morey, E., Morgans, R., Morris, S., Morris, S., Morris, H., Morselli, F., Morshead, G., Morter, R., Mottal, L., Moultrie, A., Moya, N., Mpelembue, M., Msomi, S., Mugodi, Y., Mukhopadhyay, E., Muller, J., Munro, A., Munro, C., Murphy, S., Mweu, P., Myasaki, C., Naik, G., Naker, K., Nastouli, E., Nazir, A., Ndlovu, B., Neffa, F., Njenga, C., Noal, H., Noé, A., Novaes, G., Nugent, F., Nunes, G., O’Brien, K., O’Connor, D., Odam, M., Oelofse, S., Oguti, B., Olchawski, V., Oldfield, N., Oliveira, M., Oliveira, C., Oosthuizen, A., O’Reilly, P., Osborne, P., Owen, D., Owen, L., Owens, D., Owino, N., Pacurar, M., Paiva, B., Palhares, E., Palmer, S., Parkinson, S., Parracho, H., Parsons, K., Patel, D., Patel, B., Patel, F., Patel, K., Patrick-Smith, M., Payne, R., Peng, Y., Penn, E., Pennington, A., Peralta Alvarez, M., Perring, J., Perry, N., Perumal, R., Petkar, S., Philip, T., Phillips, D., Phillips, J., Phohu, M., Pickup, L., Pieterse, S., Piper, J., Pipini, D., Plank, M., Du Plessis, J., Pollard, S., Pooley, J., Pooran, A., Poulton, I., Powers, C., Presa, F., Price, D., Price, V., Primeira, M., Proud, P., Provstgaard-Morys, S., Pueschel, S., Pulido, D., Quaid, S., Rabara, R., Radford, A., Radia, K., Rajapaska, D., Rajeswaran, T., Ramos, A., Ramos Lopez, F., Rampling, T., Rand, J., Ratcliffe, H., Rawlinson, T., Rea, D., Rees, B., Reiné, J., Resuello-Dauti, M., Reyes Pabon, E., Ribiero, C., Ricamara, M., Richter, A., Ritchie, N., Ritchie, A., Robbins, A., Roberts, H., Robinson, R., Robinson, H., Rocchetti, T., Rocha, B., Roche, S., Rollier, C., Rose, L., Ross Russell, A., Rossouw, L., Royal, S., Rudiansyah, I., Ruiz, S., Saich, S., Sala, C., Sale, J., Salman, A., Salvador, N., Salvador, S., Sampaio, M., Samson, A., Sanchez-Gonzalez, A., Sanders, H., Sanders, K., Santos, E., Santos Guerra, M., Satti, I., Saunders, J., Saunders, C., Sayed, A., Schim van der Loeff, I., Schmid, A., Schofield, E., Screaton, G., Seddiqi, S., Segireddy, R., Senger, R., Serrano, S., Shah, R., Shaik, I., Sharpe, H., Sharrocks, K., Shaw, R., Shea, A., Shepherd, A., Shepherd, J., Shiham, F., Sidhom, E., Silk, S., da Silva Moraes, A., Silva-Junior, G., Silva-Reyes, L., Silveira, A., Silveira, M., Sinha, J., Skelly, D., Smith, D., Smith, N., Smith, H., Smith, D., Smith, C., Soares, A., Soares, T., Solórzano, C., Sorio, G., Sorley, K., Sosa-Rodriguez, T., Souza, C., Souza, B., Souza, A., Spencer, A., Spina, F., Spoors, L., Stafford, L., Stamford, I., Starinskij, I., Stein, R., Steven, J., Stockdale, L., Stockwell, L., Strickland, L., Stuart, A., Sturdy, A., Sutton, N., Szigeti, A., Tahiri-Alaoui, A., Tanner, R., Taoushanis, C., Tarr, A., Taylor, K., Taylor, U., Taylor, I., Taylor, J., te Water Naude, R., Themistocleous, Y., Themistocleous, A., Thomas, M., Thomas, K., Thomas, T., Thombrayil, A., Thompson, F., Thompson, A., Thompson, K., Thompson, A., Thomson, J., Thornton-Jones, V., Tighe, P., Tinoco, L., Tiongson, G., Tladinyane, B., Tomasicchio, M., Tomic, A., Tonks, S., Towner, J., Tran, N., Tree, J., Trillana, G., Trinham, C., Trivett, R., Truby, A., Tsheko, B., Turabi, A., Turner, R., Turner, C., Ulaszewska, M., Underwood, B., Varughese, R., Verbart, D., Verheul, M., Vichos, I., Vieira, T., Waddington, C., Walker, L., Wallis, E., Wand, M., Warbick, D., Wardell, T., Warimwe, G., Warren, S., Watkins, B., Watson, E., Webb, S., Webb-Bridges, A., Webster, A., Welch, J., Wells, J., West, A., White, C., White, R., Williams, P., Williams, R., Winslow, R., Woodyer, M., Worth, A., Wright, D., Wroblewska, M., Yao, A., Zimmer, R., Zizi, D. and Zuidewind, P., (2021). Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. The Lancet, 397(10269), pp.99-111.
- Voysey, M., Costa Clemens, S., Madhi, S., Weckx, L., Folegatti, P., Aley, P., Angus, B., Baillie, V., Barnabas, S., Bhorat, Q., Bibi, S., Briner, C., Cicconi, P., Clutterbuck, E., Collins, A., Cutland, C., Darton, T., Dheda, K., Dold, C., Duncan, C., Emary, K., Ewer, K., Flaxman, A., Fairlie, L., Faust, S., Feng, S., Ferreira, D., Finn, A., Galiza, E., Goodman, A., Green, C., Green, C., Greenland, M., Hill, C., Hill, H., Hirsch, I., Izu, A., Jenkin, D., Joe, C., Kerridge, S., Koen, A., Kwatra, G., Lazarus, R., Libri, V., Lillie, P., Marchevsky, N., Marshall, R., Mendes, A., Milan, E., Minassian, A., McGregor, A., Mujadidi, Y., Nana, A., Padayachee, S., Phillips, D., Pittella, A., Plested, E., Pollock, K., Ramasamy, M., Ritchie, A., Robinson, H., Schwarzbold, A., Smith, A., Song, R., Snape, M., Sprinz, E., Sutherland, R., Thomson, E., Török, M., Toshner, M., Turner, D., Vekemans, J., Villafana, T., White, T., Williams, C., Douglas, A., Hill, A., Lambe, T., Gilbert, S., Pollard, A., Aban, M., Abeyskera, K., Aboagye, J., Adam, M., Adams, K., Adamson, J., Adewatan, G., Adlou, S., Ahmed, K., Akhalwaya, Y., Akhalwaya, S., Alcock, A., Ali, A., Allen, E., Allen, L., Alvernaz, F., Amorim, F., Andrade, C., Andritsou, F., Anslow, R., Arbe-Barnes, E., Ariaans, M., Arns, B., Arruda, L., Assad, L., Azi, P., Azi, L., Babbage, G., Bailey, C., Baker, K., Baker, M., Baker, N., Baker, P., Baleanu, I., Bandeira, D., Bara, A., Barbosa, M., Barker, D., Barlow, G., Barnes, E., Barr, A., Barrett, J., Barrett, J., Barrett, K., Bates, L., Batten, A., Beadon, K., Beales, E., Beckley, R., Belij-Rammerstorfer, S., Bell, J., Bellamy, D., Belton, S., Berg, A., Bermejo, L., Berrie, E., Berry, L., Berzenyi, D., Beveridge, A., Bewley, K., Bharaj, I., Bhikha, S., Bhorat, A., Bhorat, Z., Bijker, E., Birch, S., Birch, G., Birchall, K., Bird, A., Bird, O., Bisnauthsing, K., Bittaye, M., Blackwell, L., Blacow, R., Bletchly, H., Blundell, C., Blundell, S., Bodalia, P., Bolam, E., Boland, E., Bormans, D., Borthwick, N., Bowring, F., Boyd, A., Bradley, P., Brenner, T., Bridges-Webb, A., Brown, P., Brown, C., Brown-O’Sullivan, C., Bruce, S., Brunt, E., Budd, W., Bulbulia, Y., Bull, M., Burbage, J., Burn, A., Buttigieg, K., Byard, N., Cabrera Puig, I., Calvert, A., Camara, S., Cao, M., Cappuccini, F., Cardona, R., Cardoso, J., Carr, M., Carroll, M., Carson-Stevens, A., Carvalho, Y., Casey, H., Cashen, P., Castro, T., Castro, L., Cathie, K., Cavey, A., Cerbino-Neto, J., Cezar, L., Chadwick, J., Chanice, C., Chapman, D., Charlton, S., Cheliotis, K., Chelysheva, I., Chester, O., Chiplin, E., Chita, S., Cho, J., Cifuentes, L., Clark, E., Clark, M., Colin-Jones, R., Collins, S., Colton, H., Conlon, C., Connarty, S., Coombes, N., Cooper, C., Cooper, R., Cornelissen, L., Corrah, T., Cosgrove, C., Costa, F., Cox, T., Crocker, W., Crosbie, S., Cullen, D., Cunha, D., Cunningham, C., Cuthbertson, F., da Costa, D., Da Guarda, S., da Silva, L., da Silva Moraes, A., Damratoski, B., Danos, Z., Dantas, M., Datoo, M., Datta, C., Davids, M., Davies, S., Davies, K., Davies, H., Davies, S., Davies, J., Davis, E., Davis, J., de Carvalho, J., De Jager, J., de Jesus Jnr, S., De Oliveira Kalid, L., Dearlove, D., Demissie, T., Desai, A., Di Marco, S., Di Maso, C., Dinesh, T., Docksey, C., Dong, T., Donnellan, F., Dos Santos, T., Dos Santos, T., Dos Santos, E., Douglas, N., Downing, C., Drake, J., Drake-Brockman, R., Drury, R., Du Plessis, J., Dunachie, S., Duncan, A., Easom, N., Edwards, M., Edwards, N., Edwards, F., El Muhanna, O., Elias, S., Ellison-Handley, B., Elmore, M., English, M., Esmail, A., Essack, Y., Farooq, M., Fedosyuk, S., Felle, S., Ferguson, S., Ferreira Da Silva, C., Field, S., Fisher, R., Fletcher, J., Fofie, H., Fok, H., Ford, K., Fothergill, R., Fowler, J., Fraiman, P., Francis, E., Franco, M., Frater, J., Freire, M., Fry, S., Fudge, S., Furlan Filho, R., Furze, J., Fuskova, M., Galian-Rubio, P., Garlant, H., Gavrila, M., Gibbons, K., Gilbride, C., Gill, H., Godwin, K., Gokani, K., Gonçalves, M., Gonzalez, I., Goodall, J., Goodwin, J., Goondiwala, A., Gordon-Quayle, K., Gorini, G., Goyanna, A., Grab, J., Gracie, L., Green, J., Greenwood, N., Greffrath, J., Groenewald, M., Gunawardene, A., Gupta, G., Hackett, M., Hallis, B., Hamaluba, M., Hamilton, E., Hamlyn, J., Hammersley, D., Hanrath, A., Hanumunthadu, B., Harris, S., Harris, C., Harrison, T., Harrison, D., Harris-Wright, T., Hart, T., Hartnell, B., Haughney, J., Hawkins, S., Hayano, L., Head, I., Heath, P., Henry, J., Hermosin Herrera, M., Hettle, D., Higa, C., Hill, J., Hodges, G., Hodgson, S., Horne, E., Hou, M., Houlihan, C., Howe, E., Howell, N., Humphreys, J., Humphries, H., Hurley, K., Huson, C., Hyams, C., Hyder-Wright, A., Ikram, S., Ishwarbhai, A., Iveson, P., Iyer, V., Jackson, F., Jackson, S., Jaumdally, S., Jeffers, H., Jesudason, N., Jones, C., Jones, C., Jones, K., Jones, E., Jorge, M., Joshi, A., Júnior, E., Kailath, R., Kana, F., Kar, A., Karampatsas, K., Kasanyinga, M., Kay, L., Keen, J., Kellett Wright, J., Kelly, E., Kelly, D., Kelly, D., Kelly, S., Kerr, D., Khan, L., Khozoee, B., Khurana, A., Kidd, S., Killen, A., Kinch, J., Kinch, P., King, L., King, T., Kingham, L., Klenerman, P., Kluczna, D., Knapper, F., Knight, J., Knott, D., Koleva, S., Lages, P., Lang, M., Lang, G., Larkworthy, C., Larwood, J., Law, R., Lawrie, A., Lazarus, E., Leach, A., Lees, E., Lelliott, A., Lemm, N., Lessa, A., Leung, S., Li, Y., Lias, A., Liatsikos, K., Linder, A., Lipworth, S., Liu, S., Liu, X., Lloyd, A., Lloyd, S., Loew, L., Lopez Ramon, R., Lora, L., Luz, K., MacDonald, J., MacGregor, G., Madhavan, M., Mainwaring, D., Makambwa, E., Makinson, R., Malahleha, M., Malamatsho, R., Mallett, G., Manning, N., Mansatta, K., Maoko, T., Marinou, S., Marlow, E., Marques, G., Marriott, P., Marshall, R., Marshall, J., Masenya, M., Masilela, M., Masters, S., Mathew, M., Matlebjane, H., Matshidiso, K., Mazur, O., Mazzella, A., McCaughan, H., McEwan, J., McGlashan, J., McInroy, L., McRobert, N., McSwiggan, S., Megson, C., Mehdipour, S., Meijs, W., Mendonça, R., Mentzer, A., Mesquita, A., Miralhes, P., Mirtorabi, N., Mitton, C., Mnyakeni, S., Moghaddas, F., Molapo, K., Moloi, M., Moore, M., Moran, M., Morey, E., Morgans, R., Morris, S., Morris, S., Morrison, H., Morselli, F., Morshead, G., Morter, R., Mottay, L., Moultrie, A., Moyo, N., Mpelembue, M., Msomi, S., Mugodi, Y., Mukhopadhyay, E., Muller, J., Munro, A., Murphy, S., Mweu, P., Myerscough, C., Naik, G., Naker, K., Nastouli, E., Ndlovu, B., Nikolaou, E., Njenga, C., Noal, H., Noé, A., Novaes, G., Nugent, F., Nunes, G., O’Brien, K., O’Connor, D., Oelofse, S., Oguti, B., Olchawski, V., Oldfield, N., Oliveira, M., Oliveira, C., Oliveira, I., Oommen-Jose, A., Oosthuizen, A., O’Reilly, P., O’Reilly, P., Osborne, P., Owen, D., Owen, L., Owens, D., Owino, N., Pacurar, M., Paiva, B., Palhares, E., Palmer, S., Parracho, H., Parsons, K., Patel, D., Patel, B., Patel, F., Patrick-Smith, M., Payne, R., Peng, Y., Penn, E., Pennington, A., Peralta Alvarez, M., Pereira Stuchi, B., Perez, A., Perinpanathan, T., Perring, J., Perumal, R., Petkar, S., Philip, T., Phillips, J., Phohu, M., Pickup, L., Pieterse, S., Pinheiro, J., Piper, J., Pipini, D., Plank, M., Plant, S., Pollard, S., Pooley, J., Pooran, A., Poulton, I., Powers, C., Presa, F., Price, D., Price, V., Primeira, M., Proud, P., Provstgaard-Morys, S., Pueschel, S., Pulido, D., Quaid, S., Rabara, R., Radia, K., Rajapaska, D., Rajeswaran, T., Ramos, L., Ramos, A., Ramos Lopez, F., Rampling, T., Rand, J., Ratcliffe, H., Rawlinson, T., Rea, D., Rees, B., Resuello-Dauti, M., Reyes Pabon, E., Rhead, S., Riaz, T., Ricamara, M., Richards, A., Richter, A., Ritchie, N., Ritchie, A., Robbins, A., Roberts, H., Robinson, R., Roche, S., Rollier, C., Rose, L., Ross Russell, A., Rossouw, L., Royal, S., Rudiansyah, I., Ryalls, K., Sabine, C., Saich, S., Sale, J., Salman, A., Salvador, N., Salvador, S., Sampaio, M., Samson, A., Sanchez-Gonzalez, A., Sanders, H., Sanders, K., Santos, E., Santos Guerra, M., Satti, I., Saunders, J., Saunders, C., Sayed, A., Schim van der Loeff, I., Schmid, A., Schofield, E., Screaton, G., Seddiqi, S., Segireddy, R., Senger, R., Serrano, S., Shaik, I., Sharpe, H., Sharrocks, K., Shaw, R., Shea, A., Sheehan, E., Shepherd, A., Shiham, F., Silk, S., Silva-Reyes, L., Silveira, L., Silveira, M., Singh, N., Sinha, J., Skelly, D., Smith, D., Smith, N., Smith, H., Smith, D., Smith, C., Soares, A., Solórzano, C., Sorio, G., Sorley, K., Sosa-Rodriguez, T., Souza, C., Souza, B., Souza, A., Souza Lopez, T., Sowole, L., Spencer, A., Spoors, L., Stafford, L., Stamford, I., Stein, R., Stockdale, L., Stockwell, L., Strickland, L., Stuart, A., Sturdy, A., Sutton, N., Szigeti, A., Tahiri-Alaoui, A., Tanner, R., Taoushanis, C., Tarr, A., Tarrant, R., Taylor, K., Taylor, U., Taylor, I., Taylor, J., te Water Naude, R., Templeton, K., Themistocleous, Y., Themistocleous, A., Thomas, M., Thomas, K., Thomas, T., Thombrayil, A., Thompson, J., Thompson, F., Thompson, A., Thompson, A., Thompson, K., Thornton-Jones, V., Thotusi, L., Tighe, P., Tinoco, L., Tiongson, G., Tladinyane, B., Tomasicchio, M., Tomic, A., Tonks, S., Towner, J., Tran, N., Tree, J., Trillana, G., Trinham, C., Trivett, R., Truby, A., Tsheko, B., Tubb, P., Turabi, A., Turner, R., Turner, C., Turner, N., Tyagi, B., Ulaszewska, M., Underwood, B., van Eck, S., Varughese, R., Verbart, D., Verheul, M., Vichos, I., Vieira, T., Walker, G., Walker, L., Wand, M., Wardell, T., Warimwe, G., Warren, S., Watkins, B., Watson, M., Watson, E., Webb, S., Webster, A., Welch, J., Wellbelove, Z., Wells, J., West, A., White, B., White, C., White, R., Williams, P., Williams, R., Willingham, S., Winslow, R., Woods, D., Woodyer, M., Worth, A., Wright, D., Wroblewska, M., Yao, A., Yim, Y., Zambrano, M., Zimmer, R., Zizi, D. and Zuidewind, P., (2021). Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: a pooled analysis of four randomised trials. The Lancet, 397(10277), pp.881-891.
- Wadman, M., (2020). How does coronavirus kill? Clinicians trace a ferocious rampage through the body, from brain to toes. Science,.
- Walsh, E., Frenck, R., Falsey, A., Kitchin, N., Absalon, J., and Gurtman, A. et al. (2020). Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. New England Journal Of Medicine 383: 2439-2450.
- Wang, C., Li, W., Drabek, D., Okba, N., van Haperen, R., Osterhaus, A., van Kuppeveld, F., Haagmans, B., Grosveld, F. and Bosch, B., (2020). A human monoclonal antibody blocking SARS-CoV-2 infection. Nature Communications, 11(1).
- Wang, D., Hu, B., Hu, C., Zhu, F., Liu, X., Zhang, J., Wang, B., Xiang, H., Cheng, Z., Xiong, Y., Zhao, Y., Li, Y., Wang, X. and Peng, Z., (2020). Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA, 323(11), p.1061.
- Wang, M., Cao, R., Zhang, L., Yang, X., Liu, J., Xu, M., Shi, Z., Hu, Z., Zhong, W. and Xiao, G., (2020). Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Research, 30(3), pp.269-271.
- Wang, Z., Schmidt, F., Weisblum, Y., Muecksch, F., Barnes, C., Finkin, S., Schaefer-Babajew, D., Cipolla, M., Gaebler, C., Lieberman, J., Oliveira, T., Yang, Z., Abernathy, M., Huey-Tubman, K., Hurley, A., Turroja, M., West, K., Gordon, K., Millard, K., Ramos, V., Da Silva, J., Xu, J., Colbert, R., Patel, R., Dizon, J., Unson-O’Brien, C., Shimeliovich, I., Gazumyan, A., Caskey, M., Bjorkman, P., Casellas, R., Hatziioannou, T., Bieniasz, P. and Nussenzweig, M., (2021). mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nature,.
- Wichmann, D., Sperhake, J., Lütgehetmann, M., Steurer, S., Edler, C., and Heinemann, A. et al. (2020). Autopsy Findings and Venous Thromboembolism in Patients With COVID-19. Annals Of Internal Medicine 173: 268-277.
- Widge, A., Rouphael, N., Jackson, L., Anderson, E., Roberts, P., and Makhene, M. et al. (2021). Durability of Responses after SARS-CoV-2 mRNA-1273 Vaccination. New England Journal Of Medicine 384: 80-82.
- Williamson, E., Walker, A., Bhaskaran, K., Bacon, S., Bates, C., Morton, C., Curtis, H., Mehrkar, A., Evans, D., Inglesby, P., Cockburn, J., Mcdonald, H., MacKenna, B., Tomlinson, L., Douglas, I., Rentsch, C., Mathur, R., Wong, A., Grieve, R., Harrison, D., Forbes, H., Schultze, A., Croker, R., Parry, J., Hester, F., Harper, S., Perera, R., Evans, S., Smeeth, L. and Goldacre, B., (2020). OpenSAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients.
- Wise, J. (2021). Covid-19: New data on Oxford AstraZeneca vaccine backs 12 week dosing interval. BMJ n326.
- Wise, J. (2021). Covid-19: Pfizer BioNTech vaccine reduced cases by 94% in Israel, shows peer reviewed study. BMJ n567.
- Wu, K., Werner, A., Moliva, J., Koch, M., Choi, A., Stewart-Jones, G., Bennett, H., Boyoglu-Barnum, S., Shi, W., Graham, B., Carfi, A., Corbett, K., Seder, R. and Edwards, D., (2021). mRNA-1273 vaccine induces neutralizing antibodies against spike mutants from global SARS-CoV-2 variants.
- Wu, P., Duan, F., Luo, C., Liu, Q., Qu, X., Liang, L. and Wu, K., (2020). Characteristics of Ocular Findings of Patients With Coronavirus Disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmology,.
- Xiao, F., Tang, M., Zheng, X., Liu, Y., Li, X. and Shan, H., (2020). Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology, 158(6), pp.1831-1833.e3.
- Xie, X., Liu, Y., Liu, J., Zhang, X., Zou, J., Fontes-Garfias, C., Xia, H., Swanson, K., Cutler, M., Cooper, D., Menachery, V., Weaver, S., Dormitzer, P. and Shi, P., (2021). Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K and N501Y variants by BNT162b2 vaccine-elicited sera. Nature Medicine,.
- Xu, X., Han, M., Li, T., Sun, W., Wang, D., Fu, B., Zhou, Y., Zheng, X., Yang, Y., Li, X., Zhang, X., Pan, A. and Wei, H., (2020). Effective Treatment of Severe COVID-19 Patients with Tocilizumab
- Yang, L., Tian, D. and Liu, W. (2020). Strategies for Vaccine Development of COVID-19. Sheng wu gong cheng xue bao (Chinese journal of biotechnology)
- Yonesi, M. and Rezazadeh, A., (2020). Plants as a Prospective Source of Natural Anti-viral Compounds and Oral Vaccines Against COVID-19 Coronavirus.
- Zhang, C., Shi, L. and Wang, F., (2020). Liver injury in COVID-19: management and challenges. The Lancet Gastroenterology & Hepatology, 5(5), pp.428-430.
- Zhang, C., Wu, Z., Li, J., Zhao, H. and Wang, G., (2020). The cytokine release syndrome (CRS) of severe COVID-19 and Interleukin-6 receptor (IL-6R) antagonist Tocilizumab may be the key to reduce the mortality. International Journal of Antimicrobial Agents, p.105954.
- Zhang, W., Zhao, Y., Zhang, F., Wang, Q., Li, T., Liu, Z., Wang, J., Qin, Y., Zhang, X., Yan, X., Zeng, X. and Zhang, S., (2020). The use of anti-inflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID-19): The Perspectives of clinical immunologists from China. Clinical Immunology, 214, p.108393.
- Zhang, X., Song, K., Tong, F., Fei, M., Guo, H., Lu, Z., Wang, J. and Zheng, C., (2020). First case of COVID-19 in a patient with multiple myeloma successfully treated with tocilizumab. Blood Advances, 4(7), pp.1307-1310.
- Zhou, P., Yang, X., Wang, X., Hu, B., Zhang, L., Zhang, W., Si, H., Zhu, Y., Li, B., Huang, C., Chen, H., Chen, J., Luo, Y., Guo, H., Jiang, R., Liu, M., Chen, Y., Shen, X., Wang, X., Zheng, X., Zhao, K., Chen, Q., Deng, F., Liu, L., Yan, B., Zhan, F., Wang, Y., Xiao, G. and Shi, Z., (2020). A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature, 579(7798), pp.270-273.
Références (Générales) – Cliquez sur les liens
- Statista France: Nombre de personnes guéries du coronavirus (COVID-19) dans le monde au 23 avril 2020, selon le pays (2 Avril 2020)
- Quotidien Présent: Un virus qui n’aime pas les politiciens (16 Mars 2020)
- Psy.be: Confinement et agressivité : 1 mois pour maitriser ses pulsions et ne pas tuer son conjoint (21 Mars 2020)
- France Info: « Les vieux vont tomber comme des mouches » : à Menton, près de la frontière italienne, le coronavirus est sur toutes les lèvres (28 Fevrier 2020)
- QueFaire: Préparer sa mort, transmettre, organiser ses obsèques (14 Octobre 2014)
- France Info: Un homme de 101 ans est parvenu à vaincre la maladie. (2 Avril 2020)
- SudOuest: Gironde : à 105 ans, elle a vécu deux guerres et guéri du Covid-19 (19 Mai 2020)
- Los Angeles Times: If I become infected with the coronavirus, what are my odds of survival? (19 Mars 2020)
- France Culture: Coronavirus chinois : plus mystérieux que la peste, le paludisme, le choléra (25 Janvier 2020)
- France Info: Réaction tardive, complaisance envers la Chine… Pourquoi la gestion de la pandémie de Covid-19 par l’OMS est autant critiquée (15 Avril 2020)
- France Info: Coronavirus : visualisez l’évolution du nombre de morts dans le monde en un graphique animé (7 Avril 2020)
- Paris Match: Coronavirus : ce professeur à la Sorbonne annonçait la catastrophe (6 Avril 2020)
- France Inter: PORTRAIT – Didier Raoult, chercheur disruptif (24 Mars 2020)
- France Inter: Coronavirus : 10 façons de se dire bonjour sans se faire la bise ou se serrer la main (2 Mars 2020)
- Yale University Medicine: 5 Things Everyone Should Know About the Coronavirus Outbreak (15 Avril 2020)
- Harvard T.H. Chan School of Public Health: Coronavirus (COVID-19): Press Conference with Marc Lipsitch (4 Mars 2020)
- RTL: Coronavirus : Trump suspend sa contribution à l’OMS, une décision « absurde », selon Melinda Gates (16 Avril 2020)
- Financial Times: Donald Trump has poured fuel on the flames of coronavirus (12 Mars 2020)
- France Culture: Pourquoi le système de santé américain n’est pas solidaire (1 Avril 2020)
- Le Figaro: Aux Etats-Unis, l’épidémie semble frapper démesurément les Noirs (8 Avril 2020)
- Le Figaro: Coronavirus : pourquoi New York est-elle si durement touchée? (13 Avril 2020)
- YouTube (New York Times): ‘People Are Dying’: Battling Coronavirus Inside a N.Y.C. Hospital (26 Mars 2020)
- BFMTV: Davantage d’Américains sont désormais morts du coronavirus qu’à la guerre du Vietnam (29 Avril 2020)
- L’Express: Le chômage, l’autre tragédie américaine (28 Avril 2020)
- Oxford University Press: Breaking the Two-Party Doom Loop (24 Janvier 2020)
- Oxford University Press: Do Morals Matter? (23 Mars 2020)
- Usbek & Rica: Quand Bill Gates prédisait l’apparition d’une pandémie (17 Mars 2020)
- Red Action: Bill Gates avait averti en 2018 qu’une nouvelle maladie pourrait tuer 30 millions de personnes en 6 mois (27 Janvier 2020)
- Forbes France: Covid-19 : Pourquoi Bill Gates Reste Optimiste (1 Avril 2020)
- Ouest France: Bill Gates s’engage dans le développement de sept vaccins (7 Avril 2020)
- Oxford University Research: Covid-19 bears out the research: Music brings people together* (27 Mars 2020)
- Le Figaro: À réécouter : notre sélection de disques pour s’évader du confinement (19 Mars 2020)
- France Musique: Musique émoi de confinement 2 (3 Mai 2020)
- France Inter: Philo : Penser le confinement, cette « expérience commune » de Nietzsche qui constitue un peuple (25 Mars 2020)
- France Inter: Du plasma de patients guéris pour traiter les malades du Covid-19 : un essai clinique commence lundi (3 Avril 2020)
- France Culture: Didier Sicard : « Il est urgent d’enquêter sur l’origine animale de l’épidémie de Covid-19 » (27 Mars 2020)
- France Culture: Covid-19 : sur la piste de l’origine animale (10 Mai 2020)
- Oxford University / Oxford Martin School: China’s Announcement on Wildlife Trade – What’s New and What Does It Mean? (12 Mars 2020)
- France Bleu: Le Limousin Quentin Bontemps nous raconte le début du déconfinement à Wuhan en Chine (9 Avril 2020)
- France Inter: Comment la Corée du Sud a réussi, jusqu’ici, à dompter l’épidémie de coronavirus (1 Avril 2020)
- Oxford University Research: Digital contact tracing can slow or even stop coronavirus transmission and ease us out of lockdown (16 Avril 2020)
- Oxford University Research:Oxford scientist develop rapid testing technology for COVID-19 (18 Mars 2020)
- Oxford University Research:Coronavirus (COVID-19) Research Priorities (13 Mars 2020)
- Oxford University Research: First patients enrolled in new clinical trial of possible COVID-19 treatments (23 Mars 2020)
- Oxford University Research: Oxford COVID-19 vaccine programme opens for clinical trial recruitment (27 Mars 2020)
- Twitter (Didier Raoult): Nouveaux résultats de l’IHU Méditerranée Infection : 80 patients traités par une association hydroxychloroquine/azithromycine. (27 Mars 2020)
- Caducee: #COVID19 : Un médecin américain aurait traité avec succès plus de 500 patients avec l’hydroxychloroquine (26 Mars 2020)
- News 24.fr: Coronavirus UK: Un médecin décrit les symptômes comme «rien de tel que la grippe» (17 Mars 2020)
- Guardian: Coronavirus: UK will have Europe’s worst death toll, says study(8 Avril 2020)
- Guardian: UK failures over Covid-19 will increase death toll, says leading doctor, Richard Horton, editor-in-chief of the Lancet (18 Mars 2020)
- Financial Times: Coronavirus may have infected half of UK population – Oxford study (24 Mars 2020)
- University College London (UCL): COVID-19: UCL academics mobilise to provide critical advice and expert comment (16 Avril 2020)
- University College London (UCL): UCL, UCLH and Formula One develop life-saving breathing aids for the NHS
- Oxford University Research: Ventilator project given the green light by UK government to proceed next stage of testing (31 Mars 2020)
- Statista France: COVID-19 : quel est le statut des cas identifiés ? (24 Avril 2020)
- YouTube (L’Express): Coronavirus : pourquoi l’Allemagne s’en sort mieux que la France ? (10 Avril 2020)
- France Inter: William Dab : « Plus on retarde le travail de terrain, plus il va falloir prolonger le confinement » (11 Avril 2020)
- Oxford University Research: Universities into the breach (9 Avril 2020)
- France Culture: Jean-Christophe Rufin : « Le coronavirus méritait discussion, mais elle n’a pas eu lieu faute de moyens » (1 Avril 2020)
- Oxford University / Oxford Martin School: The world before this coronavirus and after cannot be the same: « Now is the time to start building the necessary bridges at home and abroad. » (30 Mars 2020)
- France Inter: Le confinement fait drastiquement baisser les émissions de CO2 dans le monde(mais ça ne va pas durer) (11 Avril 2020)
- Le Parisien: Coronavirus : le coup de gueule du président des médecins, contaminé à son tour (19 Mars 2020)
- Le Figaro: Masques: Macron le grand bouffon frustré souhaite «l’indépendance pleine et entière» de la France «d’ici la fin de l’année» (31 Mars 2020)
- Twitter (Nicolas Chung): Bonjour Twitter, je ne fais jamais ça mais nécessité fait loi : une amie médecin en hôpital en IdF cherche imprimantes 3D pour fabriquer les dispositifs d’adaptation pour les masques Decathlon. Merci pour votre aide et vos RT. (1 Avril 2020)
- Oxford University Research: Infectious disease experts provide evidence for a coronavirus mobile app for instant contact tracing (17 Mars 2020)
- Oxford University Research: Coronavirus Researchers at Oxford (18 Mars 2020)
- Clinical Trials Arena: Coronavirus treatment: Vaccines/drugs in the pipeline for COVID-19 (16 Avril 2020)
- l’Opinion: Coronavirus: l’Afrique suit la prescription de chloroquine du Pr Raoult (30 Mars 2020)
- Le Point: Coronavirus : une nouvelle étude de Didier Raoult sur la chloroquine (28 Mars 2020)
- Capital.fr: Les malades chroniques traités à la chloroquine sont-ils immunisés contre le coronavirus ? (3 Avril 2020)
- L’internaute: Vaccin et médicaments contre le coronavirus : le point sur les avancées (16 Avril 2020)
- La Libre.be: La Chine commence à tester sur les êtres humains un vaccin « efficace » contre le nouveau coronavirus, a indiqué mercredi le ministère de la Défense à Pékin. Il est développé sous la direction de l’épidémiologiste Chen Wei. Le vaccin a été approuvé après de premiers tests. Il peut désormais être testé sur les êtres humains. Le ministère de la Défense le décrit comme sûr et efficace, et a précisé que les préparations pour sa production en masse sont en cours, rapporte l’agence de presse espagnole Europa Press. (18 Mars 2020)
- Xinhuanews: (COVID-19) La Chine approuve trois vaccins de COVID-19 pour des essais cliniques (14 Avril 2020)
- UK Research and Innovation: Coronavirus: the science explained
- Confédération Suisse: Federal Office of Public Health FOPH: New coronavirus (14 Avril 2020)
- France Inter: « L’État ne va pas pouvoir continuer à soutenir l’économie à ce niveau-là pendant longtemps », selon le Medef (11 Avril 2020)
- France Culture: Youtube: Coronavirus : crise économique ou changement de modèle ? (12 Mars 2020)
- Le Figaro: Coronavirus : Cristiano Ronaldo transformerait ses hôtels en hôpitaux (15 Mars 2020)
- Gala: VIDEO – Didier Raoult : ce surprenant aveu fait à Jean-Marie Bigard (1 Avril 2020)
- Sputnik France: Un pilote de la compagnie aérienne AirAsia a quitté son avion par la fenêtre du cockpit en apprenant que plusieurs passagers pourraient être porteurs du nouveau coronavirus (23 Mars 2020)
- Le Figaro: Aides-soignants, caissiers, camionneurs… Les gilets jaunes sont devenus les «premiers de tranchée» (9 Avril 2020)
- France Bleu: Confinement : qui a gagné ou perdu le plus de population en Auvergne-Rhône-Alpes ? (9 Avril 2020)
- Statista France: Ces produits qu’on s’arrache en plein confinement (8 Avril 2020)
- Oxford University Research: The economic impact of COVID-19 (7 Avril 2020)
- The Conversation France: Conversation avec Frédéric Altare : l’obésité, facteur très aggravant du Covid-19 (2020)
- Science Media Centre: Expert reaction to Times Interview about vaccines with Prof Sarah Gilbert (11 Avril 2020)
- The Lancet: Sarah Gilbert: carving a path towards a COVID-19 vaccine (18 Avril 2020)
- The Telegraph: A vaccine for Covid-19 could be ready by the end of summer (17 Avril 2020)
- France Inter: Coronavirus : voici des sources fiables pour vous informer en évitant les fake news (17 Mars 2020)
- Le Point: Coignard – Covid-19 sur le « Charles de Gaulle » : une allégorie française (20 Avril 2020)
- France Bleu: Coronavirus : les dermatologues alertent sur de nouveaux symptômes cutanés (7 Avril 2020)
- Ouest France: Pour Anne Soupa, journaliste, théologienne et bibliste, le confinement ces dernières semaines a accentué notre inventivité sur la manière d’être présent (28 Avril 2020)
- Paris Match: Edgar Morin, paroles de sage (16 Avril 2020)
- Guardian: Priti Patel has said removing coronavirus restrictions in the UK will not be a binary choice and the government would not give a date for the end of lockdown. The home secretary added that five tests will have to be met before schools can reopen but said giving a date ‘would be irresponsible and get hopes up’, saying: « We want to prevent a second wave of this horrendous virus. To do that we have to ensure that we continue with the measures we have put in place. » (25 Avril 2020)
- YouTube (Telegraph): Priti Patel: « We know people are frustrated but we are not out of danger yet. It is imperative that people continue to follow the rules designed to protect their families, their friends and their loved ones; this will continue to save lives. We all want to return to living our lives as normally and as soon as safely as we can… but the 5 tests we have laid out must be met…» (25 Avril 2020)
- Le Figaro: Hervé Morin: «La reprise des cours aurait pu attendre septembre» (27 Avril 2020)
- RTL: Coronavirus : l’université d’Oxford promet un vaccin pour septembre (28 Avril 2020)
- RFI: Déconfinement en France: Martine Wonner (LaREM) : «Ce plan va être bancal faute de thérapeutique adaptée» (28 Avril 2020)
- Le Point: Déconfinement : ce qui attend les Français le 11 mai (28 Avril 2020)
- Le Point: Masque, visière, gants… Les coiffeurs ainsi que de nombreux commerces, sont autorisés à rouvrir en Suisse, où le déconfinement se fait en plusieurs étapes. (27 Avril 2020)
- Science Daily: Ultraviolet LEDs prove effective in eliminating coronavirus from surfaces and, potentially, air and water (14 Avril 2020)
- France Info: Le coronavirus vaincu par des antihistaminiques ? Certains médecins généralistes français assurent avoir guéri des patients du CoVID-19 avec des antihistaminiques. (7 Mai 2020)
- Le Figaro: Rebond de Coronavirus: Plusieurs quartiers de Pékin confinés (13 Juin 2020)
- France Inter: Karine Lacombe : “Le virus ne va pas disparaître et risque de ressurgir par clusters” (17 Juin 2020)
- Sciences et Avenir: Covid-19 : le tocilizumab efficace pour les patients dans un état grave (28 Avril 2020)
- APHP: Le tocilizumab améliore significativement le pronostic des patients avec pneumonie COVID moyenne ou sévère (27 Avril 2020)
- VOX EU: The Mauritian response to COVID-19: Rapid bold actions in the right direction [The Nobel Prize Laureate Joseph E. Stiglitz stated that the accomplishments of Mauritius are admirable and many nations should learn from them, The Mauritius Miracle (Stiglitz, 2011)] (9 Mai 2020)
- Ouest France: TÉMOIGNAGE. Des mesures « draconiennes » pour séjourner sur l’île Maurice. Jean-François Soulard, ancien élu, s’envole pour retrouver sa fille, il va devoir vivre à l’isolement total pendant 14 jours. Les contraintes peuvent surprendre mais l’île est aujourd’hui à l’abri de l’épidémie de COVID-19 (10 Janvier 2021)
- Le Figaro: «Partir quoi qu’il en coûte», les Français souhaitent s’échapper pour Pâques malgré les restrictions sanitaires (25 Mars 2021)
- Emeral Insight: Only vaccines or drugs will end social distancing (29 Avril 2020)
- Twitter (Edward Leigh): “We (UK) are an island. Why didn’t we introduce travel quarantines earlier? (9 Février 2021)
- The Conversation: Until a coronavirus vaccine is ready, pneumonia vaccines may reduce deaths from COVID-19 (14 Octobre 2020)
- Daily Mercato: “J’ai battu le Covid, mais tu n’es pas Zlatan” : le message de prévention d’Ibrahimovic (29 Octobre 2020)
- Neuroscience News: Loss of Sense of Smell and Taste May Last up to 5 Months after COVID-19 (23 Février 2021)
- New York Times: With First Dibs on Vaccines, Rich Countries Have ‘Cleared the Shelves’: The U.S., Britain, Canada and others are hedging their bets, reserving doses that far outnumber their populations, as many poorer nations struggle to secure enough (15 Décembre 2020)
- Reuters: Canada approves AstraZeneca’s COVID-19 shot, 500,000 doses to arrive next week (26 Février 2021)
- BBC: Covid vaccine: PM to have AstraZeneca jab as he urges public to do the same (19 Mars 2021)
- Politico: French government opens door to AstraZeneca vaccine for the elderly (25 Férier 2021)
- Le Point: Nicolas Sarkozy, vacciné et agacé par Emmanuel Macron (18 Février 2021)
- France Culture: Covid-19: la course contre les variants (3 Mars 2021)
- France Culture: La vaccination bat son plein dans les départements sous surveillance renforcée (3 Mars 2021)
- Le Figaro: Covid : vaccination en pharmacie «à compter de la semaine du 15 mars» (4 Mars 2021)
- Le Figaro: Covid-19: les habitants de Washington peuvent se faire vacciner directement en pharmacie (18 Février 2021)
- BBC: Covishield and Covaxin (by Bharat Biotech): What we know about India’s Covid-19 vaccines (9 Mars 2021)
- Pharmaceutical Technology: Bharat Biotech’s Covid-19 vaccine COVAXIN shows interim efficacy of 81% (4 Mars 2021)
- BFMTV: Patrick Bruel sur le Covid-19: “Faites gaffe, ce truc est une saleté” (13 Décembre 2020)
- France Culture: Covid-19 : un troisième vaccin “efficace” à plus de 90% (16 November 2020)
- Le Figaro: Le vaccin BioNTech/Pfizer peut être stocké à des températures plus élevées pendant deux semaines, selon les laboratoires (19 Février 2021)
- France Info: Covid-19 : le vaccin russe Spoutnik V est efficace à plus de 91%, selon une étude de la revue médicale “The Lancet” validée par des experts indépendants (2 Février 2021)
- Caducee: 96,4 % d’efficacité pour le vaccin anti COVID-19 NVX–CoV2373 de Novavax (14 Mars 2021)
- Doctissimo: Vaccin Novavax Covid-19 : principe, efficacité, effets secondaires (12 Mars 2021)
- Le Figaro: Vaccins Pfizer et Moderna: pas de cas suspects de troubles de la coagulation en France (19 Mars 2021)
- Le Figaro: AstraZeneca affirme que son vaccin est efficace à 79% et sans risque de caillots après des tests américains (22 Mars 2021)
- The Conversation: Vaccin d’Oxford: voici comment il a été développé en un temps record (13 Janvier 2021)
- France Culture: Covid-19 : l’Agence européenne des médicaments souligne les bénéfices du vaccin AstraZeneca (16 Mars 2021)
- AstraZeneca.com: Developing versatile immunisation programmes against COVID-19 through potential vaccine combinations (11 Décembre 2020)
- l’Usine Nouvelle: “Les vaccins d’AstraZeneca, J&J et Spoutnik sont des vaccins OGM”, explique Axel Kahn (27 Novembre 2020)
- Vidal: COVID-19: Mutations, Variants, Lignées, N501Y, E484K… de quoi parle-t-on? (18 Février 2021)
- Nouvel Obs: Des scientifiques appellent à une enquête indépendante sur les origines du Covid-19 (4 Mars 2021)
- Organisation Mondiale de la Santé: Dernières nouvelles de la part du Mécanisme COVAX à l’intention des participants concernant les retards de livraison de vaccins par le Serum Institute of India (SII) et AstraZeneca (25 Mars 2021)
- ReliefWeb: Two-thirds of epidemiologists warn mutations could render current COVID vaccines ineffective in a year or less; New survey from People’s Vaccine Alliance shows urgency of vaccinating all countries (30 Mars 2021)
- Le Figaro: Le risque d’une pénurie de papier toilette plane sur le monde (29 Mars 2021)
- France Inter: Covid-19 : 10 cartes et graphiques à avoir en tête avant le conseil de défense de mercredi (30 Mars 2021)
- Le Monde (Le blog de Marc Gozlan, journaliste médico-scientifique): Covid-19 : vaccins et nouveaux variants, quel impact ? (22 Janvier 2021)
- Our World in Data: Coronavirus Disease (COVID-19) – Statistics and Research
Danny J. D’Purb | DPURB.com
____________________________________________________
Bien que le but de la communauté de dpurb.com ait toujours été et sera toujours de se concentrer sur une culture moderne et progressiste, le progrès humain, la recherche scientifique, l’avancement philosophique et un avenir en harmonie avec notre environnement naturel, les efforts inlassables dans la recherche et la fourniture à notre précieux public des dernières et meilleures informations dans divers domaines ont malheureusement leur coût sur nos administrateurs très humains, qui malgré le temps sacrifié et le plaisir de contribuer à l’avancement de notre monde grâce aux discussions sensibles et idées novatrices, doivent gérer les contraintes qui testent même le plus fort d’esprit. Votre précieux soutien assurerait que notre travail demeure à la hauteur de ses normes et rappellerait à nos administrateurs que leurs efforts sont appréciés tout en vous permettant de ressentir une certaine fierté par notre cheminement vers une civilisation humaine éclairée. Votre soutien bénéficierait à une cause qui se concentre sur l’humanité, les générations actuelles et futures.
On vous remercie encore une fois de votre temps.
N’hésitez pas à nous soutenir en envisageant de faire un don.
Sincèrement,
L’équipe @ dpurb.com
____________________________________________________
While the aim of the community at dpurb.com has been & will always be to focus on a modern & progressive culture, human progress, scientific research, philosophical advancement & a future in harmony with our natural environment; the tireless efforts in researching & providing our valued audience the latest & finest information in various fields unfortunately takes its toll on our very human admins, who along with the time sacrificed & the pleasure of contributing in advancing our world through sensitive discussions & progressive ideas, have to deal with the stresses that test even the toughest of minds. Your valued support would ensure our work remains at its standards and remind our admins that their efforts are appreciated while also allowing you to take pride in our journey towards an enlightened human civilization. Your support would benefit a cause that focuses on mankind, current & future generations.
Thank you once again for your time.
Please feel free to support us by considering a donation.
Sincerely,
The Team @ dpurb.com
P.S.
– If you are a group/organization or individual looking for consultancy services, email: info[AT]dpurb.com
– If you need to reach Danny J. D’Purb directly for any other queries or questions, email: danny[AT]dpurb.com [Inbox checked periodically / Responses may take up to 20 days or more depending on his schedule]
Stay connected by linking up with us on Facebook and Twitter

